Abutment not seated correctly: recommendations?
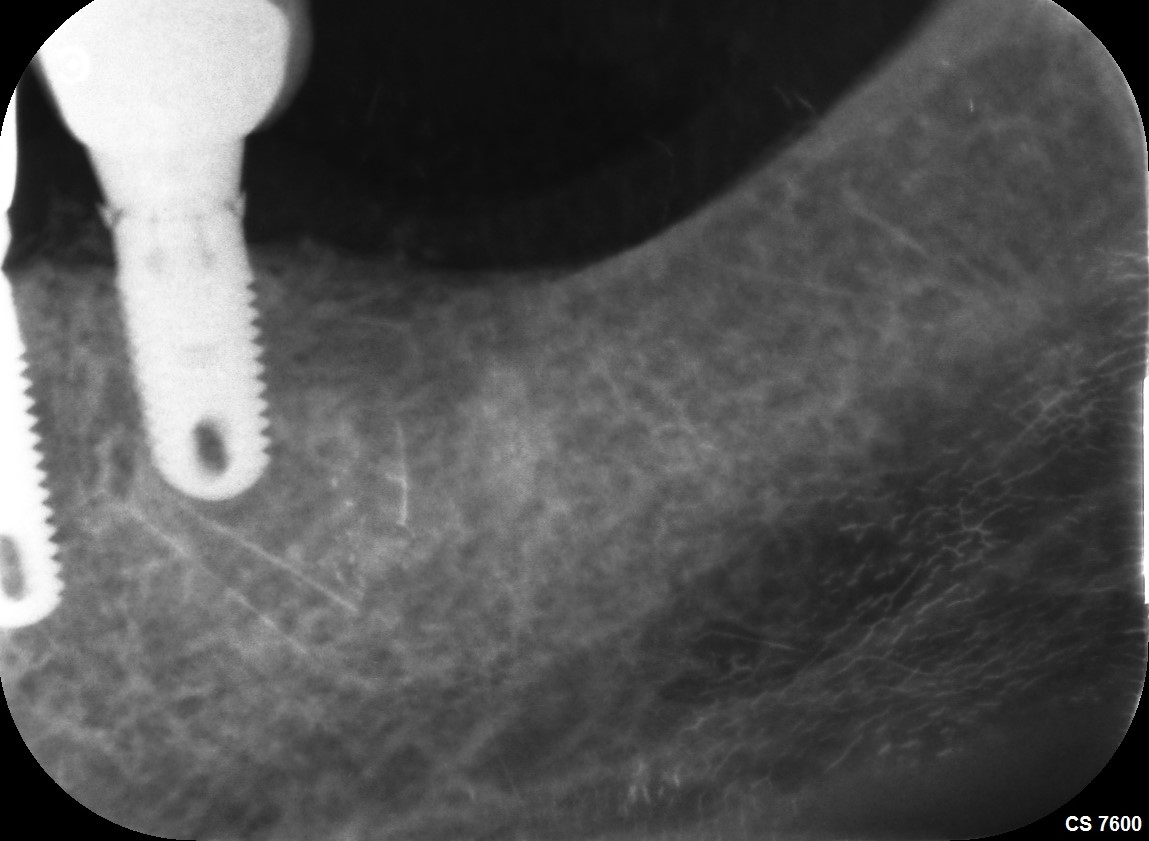
I use an implant system where I have to insert the abutment and then turn counterclockwise for the abutment to fully engage the implant fixture. To torque the abutment screw, you use a normal clockwise rotation of the torque wrench. In this case it is apparent that the abutment does not fully engage the implant platform. Should I cut off the crown, detorque the abutment and attempt to reseat the abutment fully? Or should I just leave as is which may lead to periodontal problems. What do you recommend?

16 Comments on Abutment not seated correctly: recommendations?
New comments are currently closed for this post.
Dr. Ben
8/15/2013
Thanks for sharing..
I'm not sure if the abutment OR the crown is not fully seated, i would take off the crown for two reason, first because of the gap and second i can see that there is an extra cement must be removed to avoid any further complication around the implant.
One2xl
8/15/2013
Thanks for your reply. Excess cement cleared after posted PA taken.
Richard Hughes, DDS, FAAI
8/16/2013
Dr Ben is correct. This could happen to any of us.
CRS
8/17/2013
Can I ask a dumb question if the abutment is not fully seated can the abutment screw eventually fracture? I don't restore and always hope to earn from my restorative colleagues. Will this eventually be a source for bacteria to colonize? I understand the cement issue.
Dr L
8/18/2013
Do you have a radiograph with the abutment in only? I too have the feeling it is the crown that isnt properly seated. I find, that by the time I have torqued the abutment down to the maunfacturers recommendations, it is fully seated. If youre worried about the visible space between the end of the abutment screw and the hollow bit of the implant- dont stress, thats normal.
If the abutment wasnt fully seated, then the crown would have been high in occlusion & interproximal contacts would not have be right during the trial fit. Was this the case?
Frank Avason DMD,MS
8/20/2013
Looks like crown is not seated, agree w/ Dr. L and Dr. Ben.
Dr. Alex Zavyalov
8/20/2013
If it’s clinically OK and the patient does not have any cosmetic problem, leave it, because of complexity and uncertainty the future redoing outcome. Just monitor the case.
MPE DDS
8/21/2013
I believe the standard of care dictates that a film be taken after seating the abutment to verify that it is fully seated. Then it is time to deliver the crown. New research supports that a cause of implant failure is micro-movement and subsequent "pumping" action of fluids to draw bacteria into this space. Take everything off and start over- the patient deserves better.
CRS
8/21/2013
Agree with last post implants demand a higher technical level of expertise. I think it is the abutment. If this was screw retained crown it would be easy to retrieve.
Oleg Amayev
8/24/2013
When you seat abutment, you should take x-ray before you place a crown, and then take x-ray with a crown. In your case I think abutment not fully seated. High chances of screw fracturing.
Oleg amayev
8/24/2013
Another reason crown must be replace is because looks like there is open contact between canine and implant crown.
Miguel
8/25/2013
Thank you cry much Dr. Oleg. I was inclined to change/redo crown anyways because I' won't want that in my mouth (like that). I redid a similar case like this one just this past week because the 'crown did nt seat comepletly. Wrong with a lab that did exclusively cerac. That crown was done twice. After being in mouth for less than a year, a small, it evident fistula had formed. Anyways, I removed crown, in torqued abutment, and retook final impression.
I will remove this posted case this coming Friday. The best' (excuse) for telling my patient that I've heard so far is yours. Open Contact!
I feel so much better now as crown delivered ten days ago and patient is extremely happy with procedure, her experience with how little pain she felt, and the speed of her recovery to final loading.
Thanks again. I really appreciate your time.
Miguel
CRS
8/25/2013
Miguel thank you for your feedback it shows integrity and caring for your patients. It is very helpful to know how the right lab can make or break these cases. I hope you find a good one. And the right script to tell the patient is so important so that the patient doesn't lose confidence and can accept treatment! The one year scenario of developing a fistula is very helpful information also. Often the posters don't bother to fix a problem even after they realize there is one. I think we learn when there s a consistant problem be it a lab or a failed bone graft or implant thanks for your follow up and honesty.
Miguel
8/25/2013
CRS, I thank you very much for your comments. On a side note. The crown I redid (not this posted case) I irrigated that pt with the fistula w citric acid 3% then peridex w monojet syringe prior to placing healing abutment. Do you believe there is anything else I could have done to get her healed? She recently finished a cycle of antibiotics for another procedure.
I do not have a laser yet...
CRS
8/26/2013
Since it is a mucositis without bone loss, hygiene measures should be all you need. Be careful with lasers the diode and erbium just melt tissues. The erbium is safe to use around the implant but has low penetration so a flap needs to be raised. The laser is not a substitute for good surgical technique but an adjunct to be used wisely.
Bülent Zeytinoğlu
10/3/2013
I think before going to the prosthetic step perfect fit of the abutment to the fixture has to be cotrolled.In the presented case it seems it is the crown that does not fit the abutment properly because we can see from the x ray that there is still some gap between the apex of the fixation screw and the fundus of the hollow part of bthe fixture so I think it would be better to take off the crown clean any extra cement order a new crown but please make a metal try in before ordering the outer cover.Good Luck.