Deficient Mandibular Arch: How would you rebuild it?
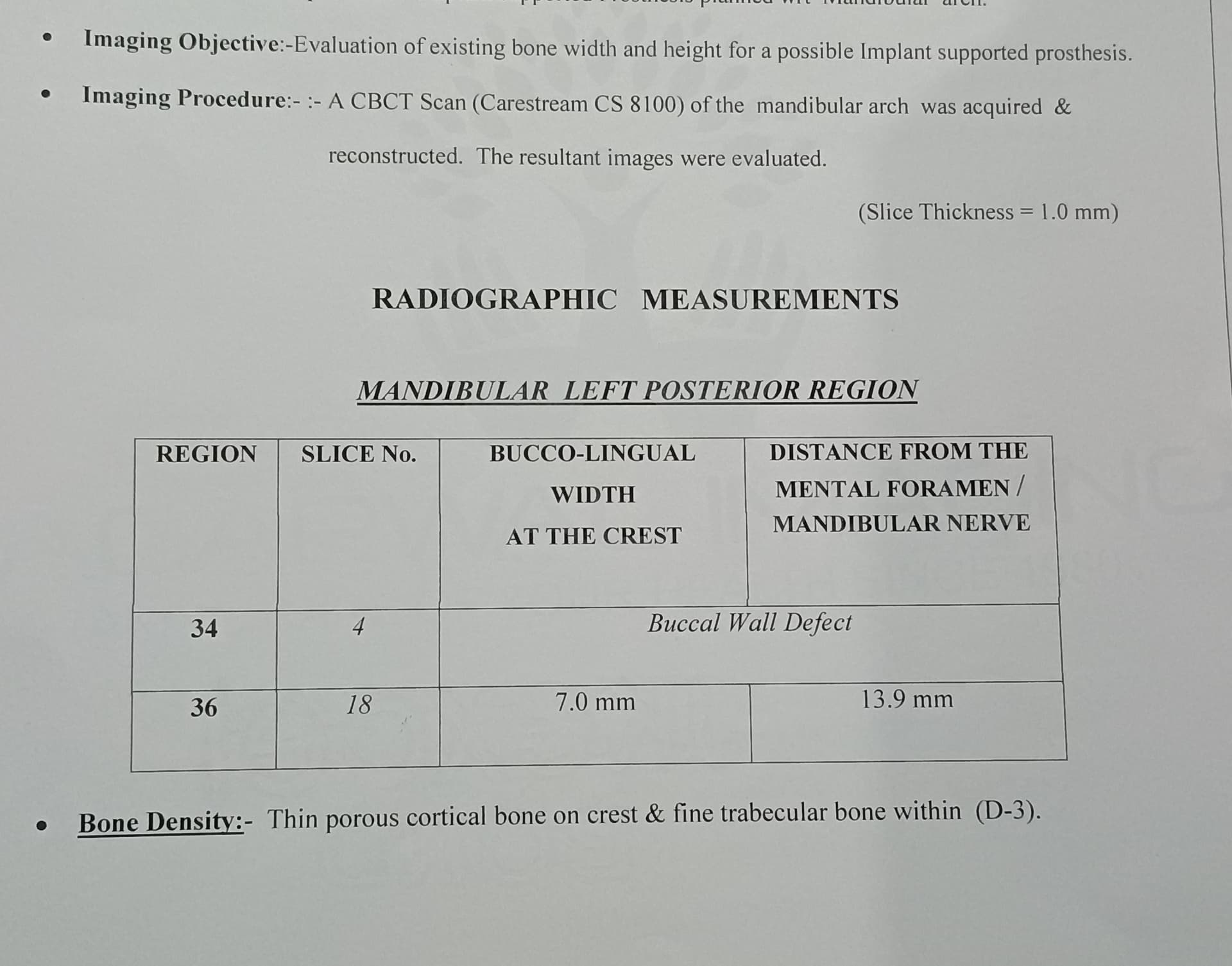
A 53-year old male patient presented at my office looking for an implant solution to missing teeth in lower right molar/ premolar region. At the visit he produced a 3 unit implant supported bridge with the implants attached. I’m looking for some options for rebuilding the bone in height and width. My concern is the proximity of the defect to the mental nerve as well as the complete lack of bone except for the thin remaining lingual portion. How would you go about rebuilding this area if at all?


12 Comments on Deficient Mandibular Arch: How would you rebuild it?
New comments are currently closed for this post.
Dr. Joe Favia
9/13/2018
I like the idea of using a J Block in this situation. I would use PRP to hydrate the block, use a screw fixation system after decorticating the entire surface of the receiving walls. I would use pericardium/collagen membrane that has been soaked in the PRP/Plasma as well. If the tissue reflected is able to reach the initial reflection site, all good for 5 months. If not, I would use a PTFE non-resorbable membrane that would need to be removed after 6 weeks during the 5 month healing phase.
Tim Carter
9/13/2018
Place one fixture anterior to the defect and the other posterior then you don't have an issue. Or you can play the regeneration/waiting game and likely be frustrated along the way.
Menachem DarwishDDS
9/13/2018
It appears that the lower anteriors have significant bone loss. you may consider extracting them and placing implants at sites 22,27,30,31. This will negate the need for bone augmentation and will yield a much better solution in the long term
Yaron Miller
9/13/2018
Thanks for your comment. What are you suggesting regarding the final prosthetic solution if I place implants anteriorly?
Menachem darwish DDS
9/13/2018
Bridge. Either screw retained or cemented.
Greg Kammeyer, DDS, MS, D
9/13/2018
I agree with Menachem that the lower anteriors should be part of the prosthetic solution. I would recommnend a monolythic zirconia bridge if you are not going to rebuild the bone. Since he beat up a 3 unit implant bridge, more implants should be planned than typical: Add one each for Males, 1-2 for bruxers and 1 for if the apposing arch is an implant reconstruction.
I would offer the choice in this situation to rebuild the bone because the defect represents where his force factors are greatest. I would use TiMesh with BMP and L-PRF. I've been very happy with the results to date versus block grafts (both autogenous and allograft blocks).
Good luck!G
Greg Kammeyer, DDS, MS, D
9/13/2018
Call me if you go the TiMesh route and I'll walk you through all the details. 623-556-5442. Greg
Dr Dale Gerke, BDS, BScDe
9/13/2018
I would ask a few questions before a reasonable answer can be given.
How long after the previous implants were lost was this cone beam/CT taken? It appears to me that bone loss is probably the result of implantitis and as such I would expect some spontaneous bone regrowth over some months (time would tell how much regrowth).
Secondly – what is in the opposing arch? If it is a full removable denture then an implant retained lower denture would be a reasonable option – or possibly a bar retainer overdenture. If the upper arch has natural teeth or implants, then a lower implant retained denture might still be an option but you could also consider an implant retained bridge.
Once these questions are answered, you can then formulate a complete treatment plan proposal (eg retain remaining teeth or extract and place implants, etc). Once you have a treatment plan you can then discuss it with the patient and see what he wants or can afford.
As an aside, if you are new to implants, doing a graft in this case might be better referred. I would suggest that if a graft is required, it would probably be best done by an experienced surgeon. It might look or sound easy but I would suggest grafting in this case has some possible issues to deal with.
Alternatively, you might not worry about implanting in the site as has been suggested by others.
I would stress it is all about the complete treatment plan. Begin with the end in mind. Plan with the overall goal decided and agreed to (by both the patient and you). It is then much easier to decide what steps are required to achieve that goal and how to go about it.
Tony
9/14/2018
All good suggestions but whatever you do the proximity of the mental foramen to the
proposed augmented sight makes it a surgical challenge.
Be careful if you go that route.
As suggested by Dale - better to use an experienced MaxFac .
Good luck - certainly a challenge
Juanes
9/14/2018
3 wall defect, I would use Sticky bone plus a collagen membrane.
Timothy Hacker DDS, FAAID
9/14/2018
Menachem Darwish DDS has a great solution and one that I have used several times with great success. You solve immediate and future problems this way. If financing becomes a problem or the opposing is a full denture use locator abutments instead of fixed. Options also include a screw retained over denture. Promising the patient more than you can predictably achieve in a short period of time is hardly ever a good choice.
oralsurgeryjj
9/19/2018
So, you wanna place implant as much as possible and avoid lawsuit from nerve damage right?
I also hate to have fixture tearing problem so I also want to place implant on at least 2nd premolar area, in which case bone grafting on the bomb defect is necessasry.
Here is the solution for you.
Check out Samuel Lee's tunneling technique in Youtube.
You would like to minimize amount of incision in order to avoid nerve damage.
So place a half inch vertical incision from crest of canine area and gently make a tunnel to the defect.
Place tunneled or rolled membrane to the area and place bone graft there....
After 3 to 4 months you might not be able to get enough bone to place an implant there, but I guess it will provide enough room to place fixture proximal to the bomb defect, at least with additional bone grafting and smallest chance to damage the mental nerve.
This is the link to Samuel Lee's youtube.
Praise and worship Samuel!!
https://www.osseonews.com/topic/techniques-demineralized-sponge-strip-and-tunnel/