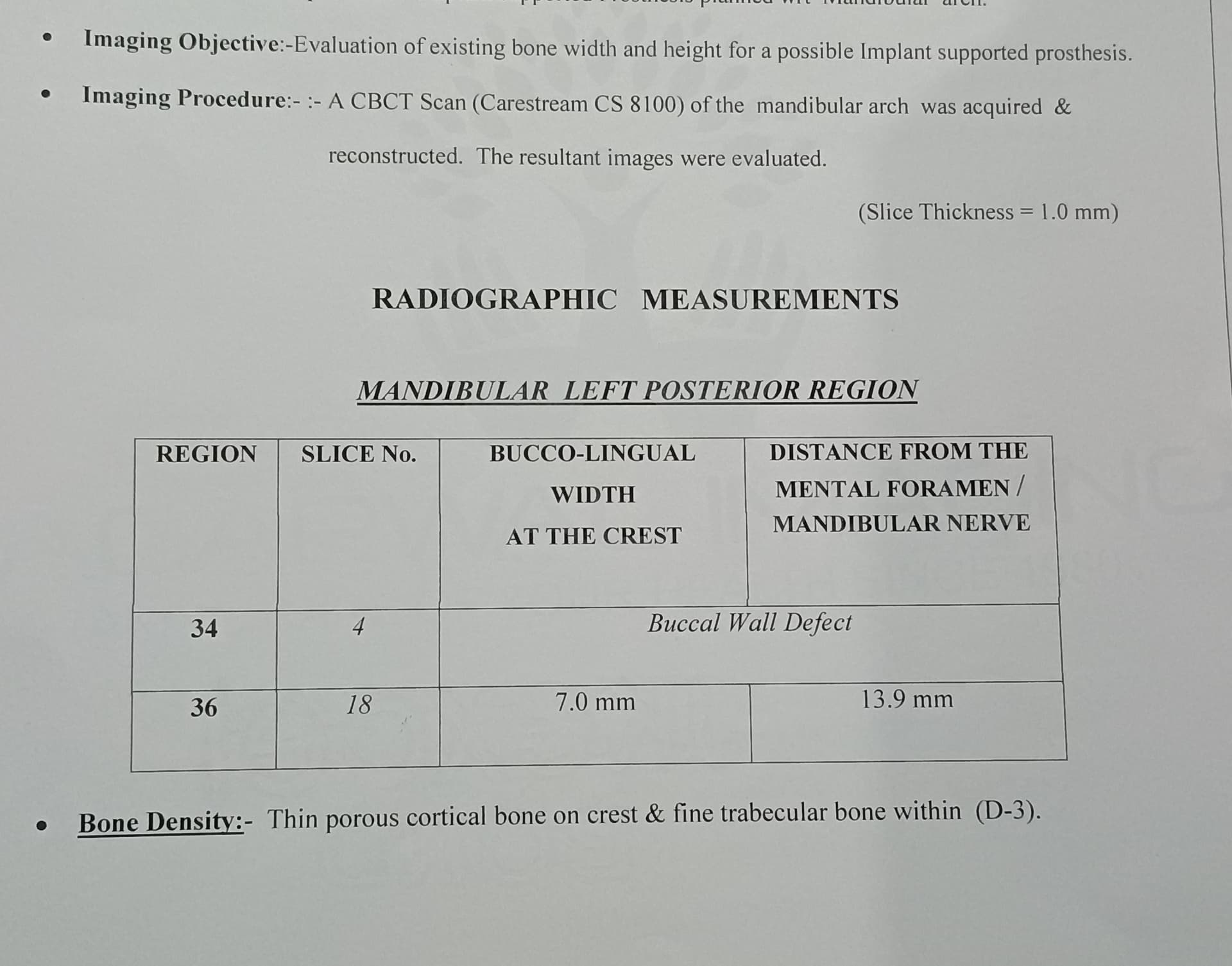
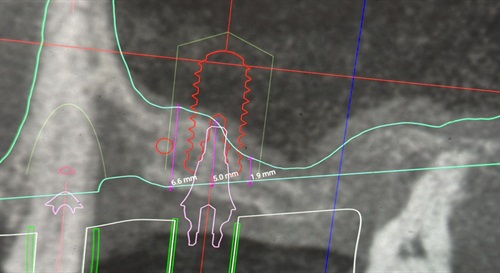
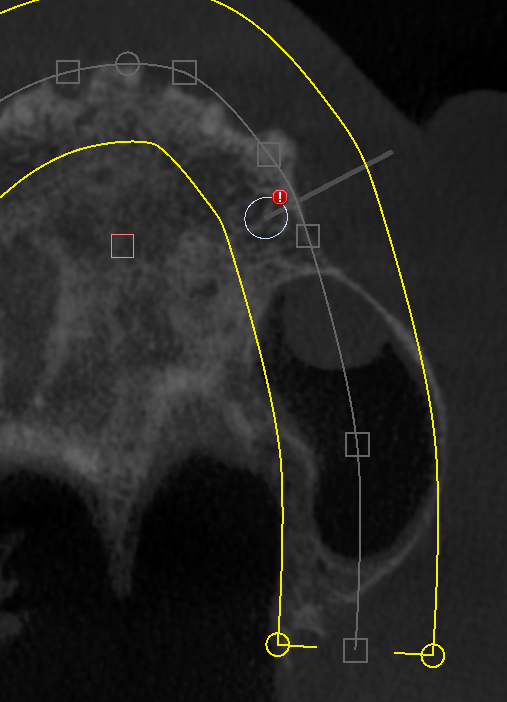
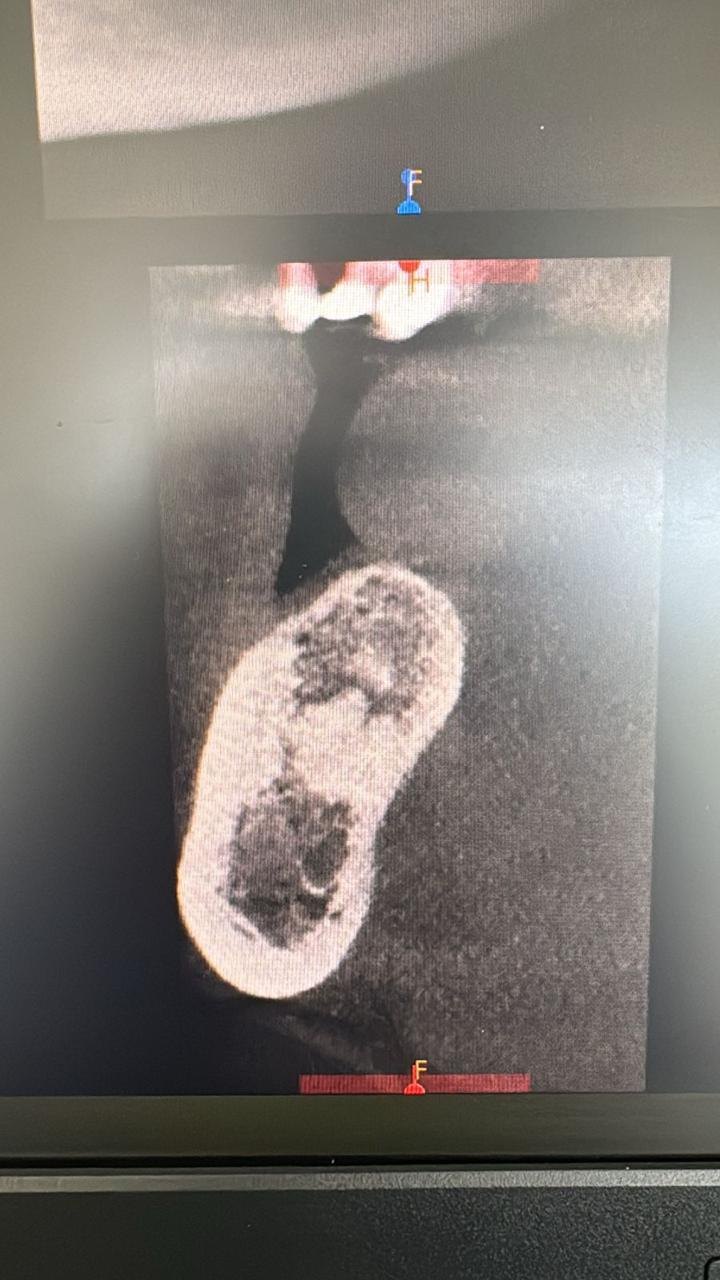
Implant breaching alveolar canal: best options?
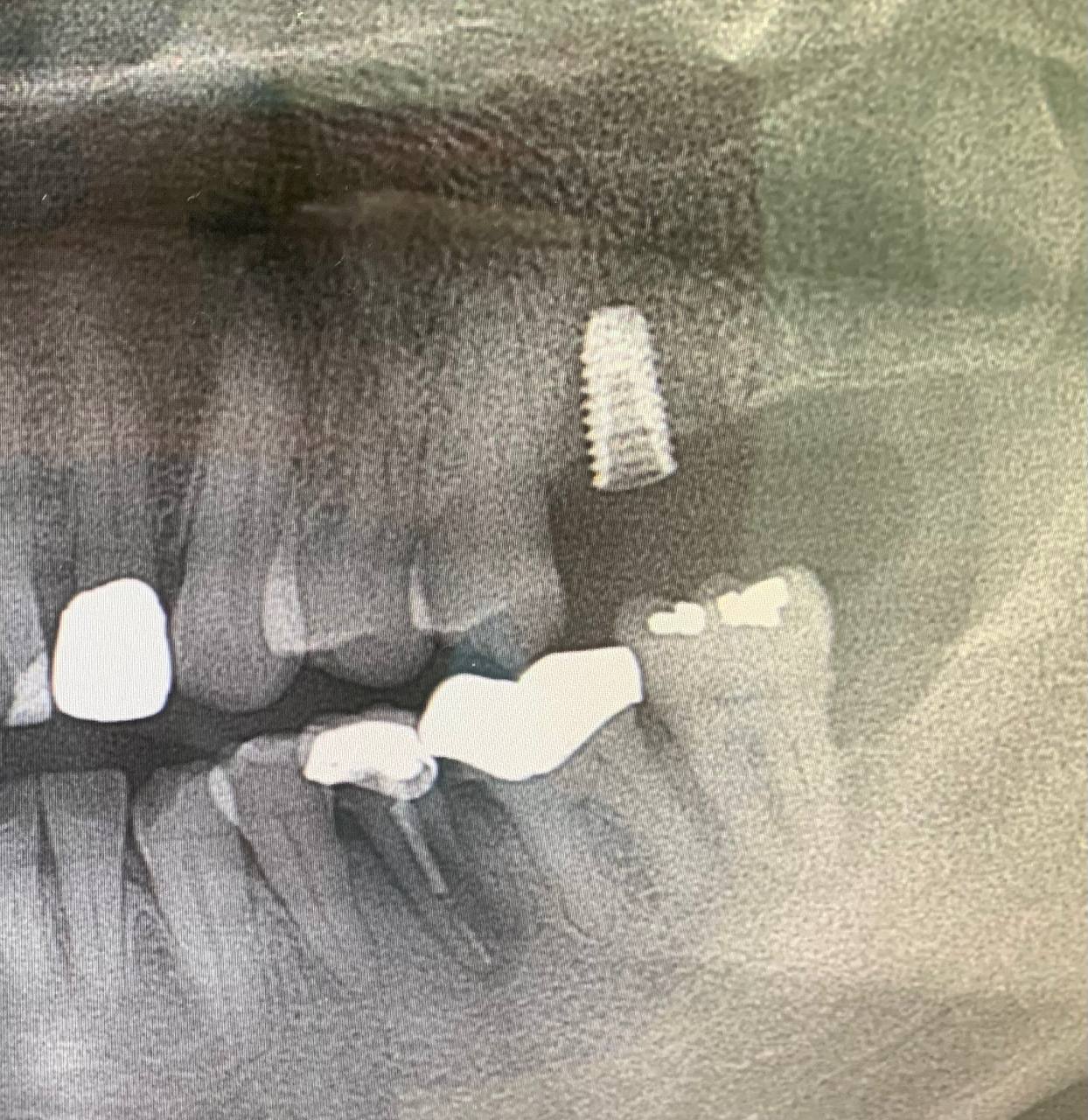
I placed an implant in the mandibular second molar site 1-week prior. A periapical radiograph shows that I have breached the roof of the inferior alveolar canal. Should I attempt to back out the implant 1-2mm or 1-2 threads? It is subcrestal anyway. What are the chances of complications if I leave it or attempt to back it out? The patient is currently asymptomatic. What do you recommend? Would appreciate feedback.

21 Comments on Implant breaching alveolar canal: best options?
New comments are currently closed for this post.
Sb oms
1/25/2016
If your patient has no paresthesia leave it alone.
On their next visit document a normal neurosensory exam.
Remember that X-rays are two dimensional,
You can not properly locate the end
of your implant and the nerve in two dimensions.
Take more intra-operative X-rays so this doesn't happen. I'd say you were lucky here.
Ken Moylan
1/26/2016
next time use an 8mm implant and you won't have to worry. Agree if symptomless ...leave alone
michael
1/26/2016
leave it alone top of ian canal is harder cortical bone most likely did not touch nerve
Alessandro aversa
1/26/2016
Platform too deep. No symptoms, leave it alone
Al
1/26/2016
I would refer the patient to an OMFS for 3D scan and his or her recommendation before Osteoinegration, just to protect yourself legally. I doubt it that anything would happen but it is the standard of care. Also the 3-D scan may show that the Roof of the canal hasn't been breached.
the other Dr.T
1/26/2016
If this was noticed at time of placement I would back it out a quarter turn, but as others have said, 2D imaging is imperfect.
As it is asymptomatic, I'd leave it.
CBCT would help.
mwjohnson dds, ms
1/26/2016
you may be actually lingual to the canal. Hard to tell with a 2D image but, since it's asymptomatic, you missed the nerve! Leave it alone.
DrG
1/26/2016
You are not in the canal. Close but not in. Asymptomatic patient confirms it. But in the future remind yourself the standard of care is to have a three dimensional image, especially in a posterior mandible.
From a legal standpoint you don't want to put yourself in a situation like this. Especially considering the alternative treatment would be to remove the failing crown behind the edentulous site and crown tooth #30 (which it clearly needs)
Leave it alone.
Dr S
1/26/2016
The standard of care is NOT a 3D image... unless of course you work for one of the big imaging companies. There is no reason to 3D image this patient pre-op.
If this is asymptomatic, leave it alone. Restore it and be more careful in the future.
Dennis Flanagan DDS MSc
1/26/2016
Get a CBCT to demonstrate that the fixture has not perforated the canal. If you back the implant out which is not a bad idea, the implant may lose stability and fail. Dennis Flanagan DDS MSc
Richard Hughes, DDS, FAAI
1/26/2016
The implant is probably lingual. You may scan to determine the location for future reference. Not all perforations of the canal result in a sensory disturbance. The nerve, artery and vein travel down the canal in a twisted manner. The nerve is on the superior aspect of the bundle about 20%of the time. So it is possible to be in the canal but not affecting the nerve.
If you choose to scan then you can subsequently act in an intelligent manner.
Dr. Howard Marshall
1/26/2016
Two points. You must immediately have qa Catscan done, and get a written report from the company which normally has a specialist advisor. Determine whether you did or did not breach the superior cortical bone of the mandibular canal, and whether there is any proximity of the implant resting on the nerve. If so, back it out. If you have not perforated the cortical housing of the nerve, consider yourself fortunate, and the patient even more so.
Lastly, do not worry about backing the implant out one turn. I have had to do that when I did not like the crestal
position, and as long as the implant is buried under the gum, it will integrate from proximity to the surrounding bone
and the normal process of bone healing next to an implant. I would wait 4 months before loading.
Krishan
1/27/2016
Thanks all for the kind guidance.I decide to leave it as such and wait for 4 months for integration.Can we expect any long term complication after loading?
Reg O'Neill
1/27/2016
For a case like this you will need to show a pre-op CT scan. for the lawyers, can you show that you took reasonable care in planning?. This I am sure is the standard of care, not doing it afterwards. Fantastic placement just wait and restore now the patient is comfortable without any complications, but I suspect you got lucky as the final outcome is a surprise to you! Looks like the mental foramen may be close by and of course the nerve bundle will be moving towards the facial which helps keep it away from osteotomies and don't forget that there may not be cortical plate protecting nerve in molar region.
Richard Hughes, DDS, FAAI
1/27/2016
Taking CBCT's are not the standard of care! The decision to take or not to take a CBCT is still up to the doctor. CBCT's do not place implants. One can still perfectly mess up a case when a CBCT has been taken. CBCT's are just another eye in the sky. They are not some magic surgical gizmo! I use them from time to time but they are not usually a requirement to perform a case.
DrG
1/27/2016
http://www.imagegently.org/Portals/6/Dental/AAOMR%20IMPLANTS.pdf
It's the recommended standard of care according to the aaoms. Try explaining to a lawyer/jury why your perspective is different. These cases when damage is done settle in the 1-3 million dollar range.
CYA
We all know what that stands for.
By the way on every CBCT software these days you can "virtually" place the implant to see if there are risks of parathesia. Maybe it's just me but why take the risk? If someone is unsure it makes total sense to just say sorry I think this might result in a nerve parathesia.
lance lindenmuth
1/27/2016
one of the first things needed is to take a periapical radiograph that is perpendicular to the tooth, bone and implant. this is foreshortened and not accurate. over and over and over we all see poorly positioned sensors or films. radiographs are certainly not an end-all diagnostic tool but are essentially worthless if not clear, concise, and done with proper angulation. don't worry and keep trying. some great advice on this case.
Dr. Best
2/2/2016
remove the implant, give cortisone if you hot the nerve, place a icon short implant!
DrMark
2/2/2016
Krishan, real quick how did the implant end up 3mm subcrestal? Did you take any parallel pin/depth verification radiographs when developing your osteotomy? Or did this happen when placing the implant? Is that a nobel active? Thanks for having the courage to share your case. Mark
ATUL SATTUR
8/17/2016
Hi.. the IOPA image is foreshortened. (You can see the lower border of the mandible). Hence, you should have atleast 2-3 mm between the implant and the canal cortex, if you take a proper IOPA. Nothing to worry about.
FES DMD
10/30/2017
I agree with Dr. G. A good plaintiff's attorney will certainly use the standard's set forth by AAOMS Parameters of Care, should a misadventure result. Therefore, next time get the CBCT prior to implant placement.