Implant bridge with little room: any comments?
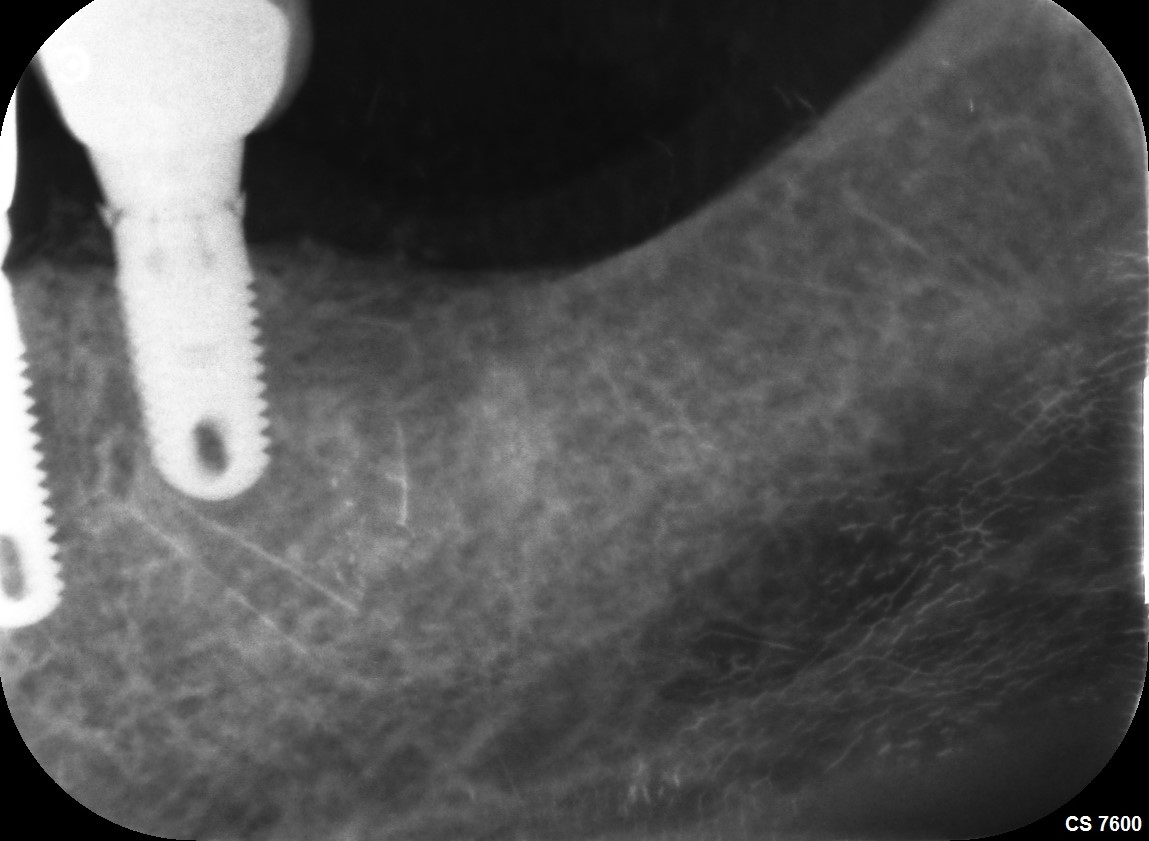
I have a 52 year old male patient who is tall and muscular. I am planning an implant bridge. Note the significant sublingual fossa. I think the best implants that I can fit in are a 4.2×8 and a 4.2×10. I will be using a surgical guide. Any comments or recommendations on my treatment plan?




18 Comments on Implant bridge with little room: any comments?
New comments are currently closed for this post.
Greg Kammeyer, DDS, MS, D
11/29/2018
Palpate the lingual as you drill to be sure you don't perforate the lingual plate.
Have you offered individual implants? You'll increase the strength of the case dramatically.
I use extra implants with men, bruxers (esp) and apposing implant supported reconstructions.
Good luck.
Mike
11/29/2018
Thanks for the comment. Good idea. I checkd the scan, the area of #21 where a third implant would be is quite narrow. Can only get a 3.2 in there safely.
Dr. Gerald Rudick
11/29/2018
I think the advice offered above is excellent. I agree with the idea of placing three implants, and all joined together in the prosthetic stage.... and as was mentioned above, when drilling the osteotomy, keep a finger on the lingual plate to ensure you do not perforate the bone...surgical guides are an excellent way to work, but they are no always fool proof..... so feel as you drill...and good luck
Peter Hunt
11/29/2018
This is excellent planning even though there is no information about the form of the restorations which might help with the placement of the implants. You are absolutely correct to do this with a Surgical Guide protocol because if you go too deep you could impinge the mandibular nerve on the anterior implant and perforate out of the mandible into the lingual region on the distal implant. There are no supports for the Surgical Guide at the distal end so it may be relatively easy to depress the Guide when drilling the channel. This might be a good case for flap exposure of the ridge and establishing a "Stop" on the bone on the distal end.
You will also need to make sure the platform of the implant is surrounded by bone if you are using an implant with a rough surface on the collar as this can easily become contaminated if left exposed . It might be safer to use an implant with a machined collar.
Every case with implantology is a challenge. You just need to work your way around the obstacles. You seem to be well on your way to doing just that. Best wishes for the case.
Sean Rayment
11/29/2018
That is a nice case and a nice presentation, although I'm not sure what the fact that your patient is "tall and muscular" has to do with the case? As with others, I would strongly recommend adding a third implant between the two you have planned. Ideally, do not line all three up but stagger if possible. That may be hard given the narrow ridge. The thin buccal plate is a concern in this case and you may experience buccal recession and bone loss as a result of not having a thicker plate. Best of luck.
John
11/29/2018
Two Stage Split Ridge procedure works well on this case type. It’s like creating a sideways “rumble seat” when you flip that Buccal plate out at the insertion appointment. You get that Buccal cortical plate reinforcing what’s usually the weakest point on thin mandibular ridges.
You also gain 3-5 mm attached tissue over Ridge crest as it heals. And the final prep can be done gently with hand or non-aggressive powered drills which allow feeling of the bone site.
Bicon has short Implant’s to sit passively in the preps, as well as side-cutting only and end-cutting only bits of hand or powered driven nature. You can’t penetrate the side nor inferior cortical plates in normal use.
Dennis Flanagan DDS MSc
11/29/2018
Check the bite load of this patient to determine his maximum bite capability. He may have a 300N capability. If so, it would be better to place 3, 3.2 diameter implants as long as possible and splint for excellent support.. Don't forget we need 2mm F and L bone thickness for a long term functional outcome.
Timothy C Carter
11/29/2018
Once again it amazes me the stuff that docs seek advice on. I think you are good to go with your plan but you should have the confidence to move on without seeking the input of a bunch of armchair quarterbacks. Obtain the necessary skills and confidence to move forward with treatment or refer to another doc. Patients deserve better than a bunch of weekend trained folks looking to increase production.
Sean Rayment
11/29/2018
Mentorship, one person getting help or learning from someone with more experience. This is an excellent case to discuss both from a surgical and restorative perspective. How many implants, what type of surgical guide, splinted or single units? Lots of interesting threads.
michael johnson dds, ms
11/29/2018
Dr. Carter, you crack me up! It's what a lot of us are thinking. Thank you for articulating it. The plan is sound. To quote Nike...Just do it. As for the weekend trained folks, I just conferred with an attorney, trying to keep a practitioner out of litigaton, and he calls them "amateur implanters" and are a steady source of revenue for him. So follow Dr. Carter's advise and treat what you're comfortable with and refer what you're not comfortable with. Thank you for your case presentation and your treatment planning is sound.
Carlos
11/29/2018
Dr. Carter and Dr. Johnson, why are you here ? We are here to either learn or teach those who are starting. I guess that you both were born knowing how to place implants. I bet that both of you had questions like this type. You have to start somewhere and this doctor is trying to get some feedback.
As a matter of fact, if you have read the answer of some of our colleagues, they have different versions on how to work this case.
May I suggest to you too to go to a page or site where your intelligence are not insulted !!
I can’t believe your humbleness!!!
Dr. Moe
11/30/2018
Carlos, I agree 100% with you. We are all here to learn, if you are too high and mighty (Dr. Carter and Dr. Johnson) , why are you guys here with us lowly "weekend course implanters"? So you can feel good about yourself and give your little egos a boost? Or maybe your are just envious that us G.P.s are doing implants and taking away production from you? And How do you obtain confidence? Oh wait it by doing more and more cases that are just outside your comfort zone. Hence asking for guidance from more experienced colleagues.
Like Carlos said, maybe you guys knew how to place every implant in perfect place with perfect results the day you two were born, however most of us cannot. So we need guidance and ask humbly for it, we DON't need your snide remarks, so you can feel better about your ego.
Please refrain from answering if all you got is a sarcastic, demeaning remarks. No one needs to hear your negativity or find out about how Great a doc you are to see all the issues even before we mortals can think of it.
Sharon
11/30/2018
Good response.
DrD
11/29/2018
Good comments on this case. My suggestions: 1. I think the fact this is a big muscular guy is significant. Because of this, in combination with the thin ridge, I would not consider a bridge here. I would place individual implants, or you will have screw loosening issues, bone loss, or even implant fracture with narrow implants. 2. Because of the above, also, use the widest diameter implants you can . See if you can get 4 mm implants in each site. 3. You mention using a surgical guide. What type of guide? If you are talking about a “positioning “ guide, I think you have difficulty. With the narrow ridge, and nerve position, there is no room for error. This is clear looking at the CBCT scan and your planned implant positions. With a positioning guide there is more room for error than you might imagine and than I would want, and I’ve been placing implants over 30 years. That’s great to palpate the lingual plate, until you feel the drill come through. This case is a clear indication for a CBCT generated fully guided splint case. Those implants need to go right where you planned, and that is the only way to do it.
My $0.02.
Sharon
11/30/2018
Very helpful $0.02 worth!
John
11/30/2018
With Two Stage Ridge Split, I usually place 4.5x6.0 implants in this narrow ridge type. I concur with DrD on the preference for at least three implants on this case.
Mick
11/30/2018
I am doc that posted this case. Interesting comments. First....I am not a young doctor. I have 40 years experience....6 years doing implants....have placed over 200. My objective is to do what is best for my patients.
I have a CBCT in my office...I have an Ostell RFA unit. I am a Fellow on ICOI This is a challenging case due to limited space for implants and narrow ridge and physiognomy of pt.....strong large man with presumably forceful occlusion. As has been suggested, I agree that 3 implants would be better. However, the site for the 3rd implant has a too narrow ridge. Thanks to the comments of you guys, I decided to refer this case to OMS for implant placement. There was a comment made that doing cases outside of comfort level is the only way to learn....totally agree. The determining factor is to do what is best for our patients. Thank you for all comments
This site is an excellent resource for bouncing ideas.
Mick
Angela
12/1/2018
Use Bicon implants . you can easily place 4x5 there. I recommend doing it guided