Implant placed into extraction socket: thoughts?
I was wondering, in general, what the consensus opinion is here about placing an implant into an extraction socket that is 6 weeks old. What is your protocol? Would you graft around the implant? Do you do the surgery in one stage or two stages?
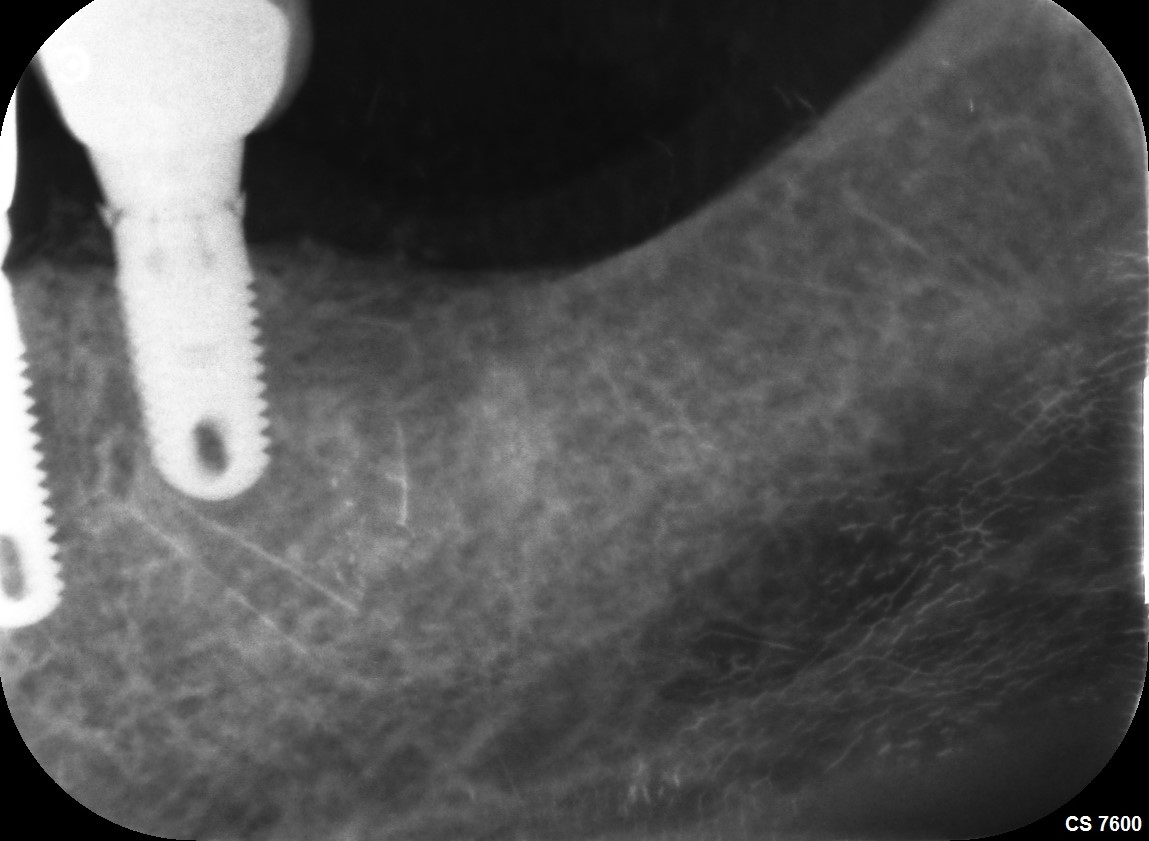
 wide platform implant placed, single stage surgery, no grafting material used.
wide platform implant placed, single stage surgery, no grafting material used.
32 Comments on Implant placed into extraction socket: thoughts?
New comments are currently closed for this post.
Sb oms
6/30/2014
In my hands a bone-implant gap of greater then one mm gets grafted.
So in a molar extraction socket, the bone-implant gap is bound to be greater then one mm both towards both ends of the socket.
At six weeks you don't bone in an extraction socket. So again, in my hands, all the soft stuff gets scraped out and the defect grafted. I'm sure there are other opinions on this matter.
Regarding one vs two stages, that's an issue of primary stability. If it's stable, one stage. If not, bury it. At six weeks you will have enough soft tissue to do either.
Now, regarding the case above, which I'm sure your going to get beat up for,
Here are my thoughts:
1. This is a true disservice to this patient. You have created an unnecessary cantilever and food trap. You placed the implant in the distal root, and the implant basically comes up into the molar behind it. Whether you graft the implant-bone defect is irrelevant, you've already created the problem by placing the implant here. I'm only looking at this in two dimensions from your x-Ray, but even in two dimensional analysis you are way off. Did you see this with your check films as you were working on this?
2. If you are going to place an implant into a molar socket, you need to be in the middle, just like any other site. This requires adequate bone and surgical technique. Your placement is too far to the distal, and this is likely to cause problems down the line.
3. Always root plane the adjacent teeth when placing implants. There is a huge chunk of calculus on the distal of the anterior tooth. This makes me cringe, and I'm not even a periodontist.
4. I know you asked about grafting gaps, and you didn't ask for this, but I'm gonna share something I've learned. You waited 6weeks to place this implant. I'm guessing you had no bone in the socket, and this is where your implant ended up. If you had waited an additional 10 -12 weeks, you probably would have had a much easier time at placing this implant in a better position. So my advice, slow down, and make it easy. This is a non-esthetic case. There is no rush.
Immediate molar implants are challenging, and they require certain skills that take time to master. Your correct in asking about the gap issue, it is a concept that is in flux, and we really don't quite know in many cases what is correct.
Adam
7/1/2014
Thank you for your feedback, I am aware it is less than ideal placement and plan to correct placement issues with future implants, I was disappointed with placement m-d. It was my first post extraction and the drill did slip. I new to the grafting game and have some courses lined up so am asking for experience on when and timing post extraction which you have answered more than adequately.
Peter Fairbairn
7/1/2014
Hi Adam , that has happened to me as well and the cases are restored but not ideal but acceptable .
Your case looks good Sb Oms has just given good advice to mull over we are all always learning.
All the best.
Peter
Peter Fairbairn
7/1/2014
Very good synopsis sbOms , of a difficult area the lower 1 st molar . The preservation of tissue can be important here both hard and attached soft tissue for long term success .
But as you said requires a bit of skill to place accurately into the inter-radicular bone as well an understanding of grafting protocols and materials.
Peter
Richard Hughes, DDS, FAAI
7/1/2014
Sb OMS and Peter make valid points. I usually graft these sites with a particulate (OsteoGen) or if infected I give it tincture of time and revisit later and treat accordingly ~ graft and or implant. To place an immediate implant in these sites is tricky.
doctor x
7/1/2014
In mine opinion is best placing 2 implants for a molar.and never destroy the Sept in the middle or drilled ..
Checkout the nerve position can you give us a bigger picture Panoramic or much lower the Rx
Have a nice day.
Nitin Sharma
7/1/2014
Sorry to mention and disappoint you, the implant might fail. See the implant Bone interface where u may notice radiolucent margin at distal surface of this implant and otherwise a big challenge as prosthetic outcome. Y not do a good socket preservation if possible, otherwise place the implant at the mid interseptal area and possibly Graft all around.
Jaw doc
7/6/2014
The distal radiolucency doesn't matter if this is an immediate post-op radiograph. Implant will osseointegrate. Restoration, though less than ideal, will still be acceptable/functional.
Stanley Sargent, DDS FAGD
7/1/2014
I tell the patient that these are very difficult immediate implants to do. They are informed that if I don't get enough torque with the implant I will change plans and do socket preservation.
After careful removal of the tooth, and other pre-osteotomy procedures (socket curettage, bone graft prep with patient heme, etc.) I always start with a precision drill and go straight into the furcal bone. Drill the osteotomy like normal from there. Always graft all spaces. I always place a PTFE or Amnion/Chorion membrane over site.
adam
7/1/2014
Thankyou all for your comments, I don;t mind all feedback as one learns from mistakes better than successes.
tareqsayed
7/1/2014
MY OPINION ,OSTEOTOMY SITE IS MIDINTERSEPTAL PLUSE PARTICULATE GRAFT ALL AROUNDTHE IMPLANT &THE SITE COVERED BY PTFE MEMBRANE.
lyle
7/1/2014
there is an article which came out a year or so ago by dr. tarnow and chu about bone grafting the gap. no need to in the posterior. osteoblast can not differentiate 1mm or 2mm or 3mm so to simply state to bone graft if the gap is Xmm or more is simply to make the surgeon feel good. think about an extraction socket which is say 10 or 12mm across, does the osteoblast reach only 2mm? no the entire socket will heal. i haven't bone grafted the gap in years and the bone fills in nicely. however when you do an anterior case or if part of the wall is missing then a bone graft is indicated. when considering immediate placement, you also need to take into account socket healing and the changes which come along with it, namely bone loss or shrinkage. also the area of the mouth makes a difference as we know the facial plate on the upper anteriors are <1mm in 95+% of patients. you will need 2mm for longterm stability. also take into account your implant surface, thread pattern, and the ability to place the fixture subcrestal will help in considering immediate placement. i do immediates whenever anatomy allows and the success rate is no different. in fact in the esthetic zone there is no better way to do it unless the facial crestal plate is blown out.
Jaw doc
7/6/2014
I agree that the socket spaces will eventually fill up with bone anyway. But grafting will help preserve bone height & width better, in most cases.
alex corsair
7/2/2014
Placement of an immediate implant in a molar extraction socket is generally a poor risk to benefit scenario. Placement in the socket of a single rooted tooth at 6 weeks post extraction v. immediate? This might be indicated if the extraction was traumatic, if infection was present or if more gingiva was required. Then at 6 weeks primary closure could be obtained if grafting was indicated. Gaps larger than 2 mm should be grafted especially in the esthetic zone. The implant would integrate without grafting but facial bone loss could compromise the esthetic result. In fact in high risk esthetic cases it is more predictable to graft and then place in a fully healed site. In other cases immediate placement and provisional restoration can be successful.
CRS
7/2/2014
Just remove it, graft and replace you'll avoid chasing the complications and additional visits in the future. You're gonna lose money on this one chalk it up to experience and do the best for your patient. It's your patient I assume they trust you. Good luck thanks for posting.
rsdds
7/2/2014
I would leave it alone not ideal but we all have made mistakes like this and most of them are still in function.. next time take a cbct this is a dangerous area to use this lengthy implant.. I own a cbct and you'll be surprised how many mandible concavities I've seen in this area
CRS
7/5/2014
Some very excellent points, the implant looks too long getting close to the canal. But listen to, we all make mistakes and they are still in function? What's the point of taking a post op film if the result is not corrected? The implant could have been angled slightly to come out in the middle of the socket, Nobel active is a nice way to go. Now you will need a custom abutment etc on a straight forward grafted case with delayed placement. As a dentist one should be able to line up an implant for draw and ideal restoration. Now you have a bunch of posts to correct an implant placement which was iatrogenic. Seems backwards to me. That's why I mentioned the loss leading, if another surgeon placed this for you I don't think you would be too pleased.
dr Fux
7/2/2014
If I've got it right, a wide fixture was installed. Is there a possibility to design premolar crown with premolar pontic cantilevered mesially? To develop modified ovate pontic site during uncovering and emergence profile development, to prevent food trapping issues. A wide platform could, maybe, survive mesial cantilever?
Don Rothenberg
7/2/2014
First off, I think this implant will be fine... you will just need to design the abutment and the crown so that there will not be a trap for food.
If the tooth was already extracted I would wait until full healing (4-6 months)...then you will have ideal implant placement.
It is important to take a "check film" to verify the location and angle of the implant and correct it to the middle, if necessary. With more experience you might not need to on every case but we usually do.
As of late, if the tooth is still in...I will hemi section the molar and drill through the middle with a pilot drill...and 1 size up (2.5mm)...
We will then carefully remove each root ...do the final osteotomy drilling and place a shorter 6 or 8 mm implant.
We have also been using A-PRF membranes (with or without mineralized FDB)...to fill the gap and cover the surigal site before suturing. The PTFE sutures will remain in place for 2 weeks.
I see no need to immediately load any posterior implant...we wait 3-4 months before placing the abutment.
This case brought up a lot of good questions...and ideas. We all do this work a bit differently and it is great to hear what other folks are doing.
Let us know how the case turns out...I'm sure the patient will be happy with the result.
Thank you all !
Zaki Kanaan
7/2/2014
Adam, whilst I agree with most of the very useful comments above and that this implant 'may' not have integrated, is in a less than ideal position and perhaps should have been grafted or even buried....don't beat yourself up about it. We are all learning and continue to do so. There have been some studies suggesting that placement of implants distally in a molar site and shaping the overlying molar tooth into 2 premolar units (into an anterior cantilever situation) can still be successful. This is similar to 2 missing premolars with a reduced mesiodistal width where 2 implants won't fit and a single implant is placed. A centralised implant is still my preferred choice and although not ideal, it can still work.
Vipul G Shukla, DDS
7/2/2014
Yes, placement is not ideal, but you can work with this. A skilled lab technician can help you down the line. Give a very wide mesial emergence profile to the crown and avoid unsupported porcelain. You could have trouble with the seating of impression coping.
Two good points, as seen on this X-ray:
1)At least 2mm of apical solid bone was engaged, and looks like...
2) sub-crestally placed, as it should be.
Is this a MIS SEVEN wide platform implant?
adam
7/2/2014
yes a wide platform seven, as I had the available bone before the IAN as seen and check on a CBCT (always taken for any implant) the 11.5mm was selected so that a good 2-3 mm of bone could be engaged past the extraction socket for primary stability, about 35-40Nm was achieved primary stability. Position disappointing but primary stability was good, and a cantilevered two premolar or a crown well made as it will be a screwed retained single unit with a divergence profile starting from the implant head (as always particular skill from doing a lot of anterior cosmetic work to get appropriate gingival shape), even with a single crown the food trapping will be easily managed he has very thick tissue. the cantilever may create more. I will trim the mesial of the seven, the P-b position is good and it will have a nice central screw hole. I after restored many implants over the last ten years so restoring it is not a problem but I have just stated placing implants, this was my first in an early extraction socket.
Thankyou for your feedback everybody.
jaime
7/3/2014
Hi Colleagues ,
I´m south african trained dentist and specialized in Sweden in implantogy ( Very conservative )
Portugal has about 25% of trained Brazilian dentists . I am surprsed at what I´ve seen with success especisally regarding Zygomatc Implants which to me is a speciality and not to all MFOS .
WE have alot to learn with the adventurous Brazilian dentists due to various factors .
In my opinion , rather have a pontic mesially placed rather than in the center.
It´s two schools of thought not mentioning other cases !
Best Regards .
Peter Fairbairn
7/3/2014
Placing into the distal socket is protocol at some teaching institutions ....not mine though .
Immediate placement into the bifurcation with grafting both root sockets after a 3 week soft tissue healing period is my protocol here ,generally do a case a week like this .
Like golf takes a bit of practice ....
As they say the only Implant "failures " are the ones done by other dentists..
Peter
Kevin
7/4/2014
Do not remove this implant if healing and integration are proceeding well! As many above have said, is placement ideal?...no. But are you doing your patient a disservice by working with it?...no! Comfort, fit and function will a be fine if you have a custom abutment made and the final restoration is kind to the soft tissues. I give most of my implant patients a Waterpik which aids in cleaning around even the most perfectly placed implants which still trap at least some food.
Adam
7/4/2014
Yes I agree with you as this was my own assessment and criticism of my own work, I was really enquiring about the bone grafting etc and whether if people graft they carry out single stage surgery or two stage surgery, thank you for your real world feedback.
Osbert Usher
7/6/2014
All the above comments are valid. Everyone can look at something from a different point of view, and they may be right.Yes, this implant is more distal than it should be, but I also believe that it can be restored and not putting the patient through another surgical procedure. Of-course, it should have been done right. Considering that this is in the molar region and poses little or no aesthetic problem; why not wait for healing to thoroughly occur before placing implant.Life would have been easier and less possible complication. Like Kevin, we suggest the use of a waterpik after every finished implant.
Your Implant will work Adam.
Dime Sapundziev
7/8/2014
Implant is good and the final result won't be acceptable it will be exellent with appropriate abutment selection and final crown design.
For all Mr Perfect's and x-ray lovers I have some questions. What do we want to achive with these implant, function or esthetic? What is estheticaly acceptable for us and functionally not acceptable to the patient? Are we doing dental implants to have a good x-rays?
Implant is ok, instruct the patient to take good care for it and that is it.
Too much philosophy for a good case.
Plese post it after couple of years.
For those that consider to restore a molar with two implants I think that there is a great leak of understending of basic principals of dental implants and osseointegration.
DrT
7/8/2014
In answer to your question..What do we want to achieve?..my answer is LONG TERM HEALTH. With implant placement like this, there is going to be an over-contoured crown mesially. This will result in an area that will always be a challenge to both the patient as well as the hygienist to clean properly. Furthermore, if this patient has a previous susceptibility to inflammatory periodontal disease, then this compromised implant site will in all likelihood have an increased susceptibility to develop peri-implantitis. Just in case you have not been keeping up with the literature, we are seeing peri-implantitis in an alarmingly high number of implant cases. So, in this case, I am not concerned about the esthetics, and I do not care one bit about an x-ray...what I am concerned about is the LONG TERM HEALTH of some treatment that this patient has spent quite a large amount of money on, and which he is expecting to be maintainable and healthy for many hears. Can you assure him that this is going to happen given the current position of this implant fixture????
CRS
7/10/2014
Actually I agree with you, the poster placed way too long of an implant and got lucky not injuring the nerve. The implant is too close to the distal molar and there is a cantilever, food packing area on the mesial. I extract and graft then place the implant where it needs to go, in the middle of the alveolus. In the long run 12-16 weeks for graft healing for an implant that should be in place 20 years is a good bet. And there is significant literature on implant failure I think it is because corners are being cut.
adam
7/8/2014
thankyou for your comments I am glad somebody else feels the same way.
Dr. Gerald Rudick
8/12/2014
Adam, look at the attention you received!
A lot of good advice and suggestions were given. Judging by the xray, I do not think this is a hopeless case....true, it would have been better had the implant been placed more in the middle of the space....but there are thousands of implants that have survived very well being placed in the distal root socket, and have a properly contoured easy to maintain crown......... the implant is a little too long, but you do not report any paresthesia, so this is positive.
Next time you do one of these cases, just take more time, and do a bone graft...wait six months and place the implant in the most ideal position....consider this a learning experience, and I am sure your patient will appreciate the concern you have given this.
Gerald Rudick dds Montreal, Canada