Is this implant too close to canine tooth 23?
I installed an implant in the site adjacent to #11 [maxillary left canine; 23] without any overt problems. However, after I took a radiograph to check the position and angulation I noted that the implant was very close to the natural tooth root. I showed the radiograph to a few specialists and they recommended detorquing and removing it before it became osseointegrated. Should I wait and see if any complications develop or should I remove it right now?
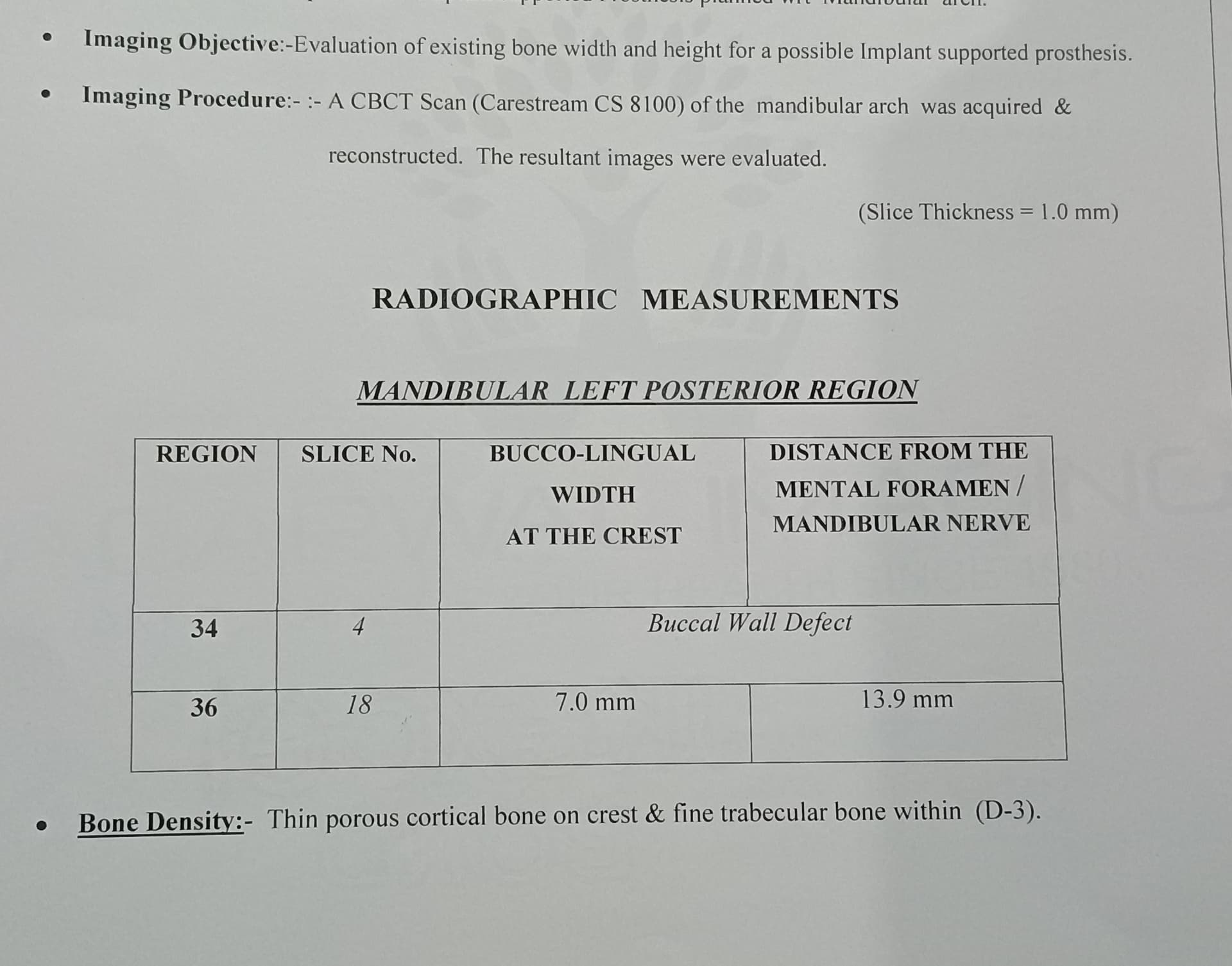
![]Implant in 24 region](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/11/image.jpg)
Implant in 24 region
37 Comments on Is this implant too close to canine tooth 23?
New comments are currently closed for this post.
CRS
11/4/2012
Remove it the implant is on an angle and will be difficult to restore. Did you use a surgical guide? A cone beam would give a better view but based on this film the implant is not aligned with the adjacent tooth and there is plenty of distal bone.The implant is crooked
Peter Fairbairn
11/4/2012
They are right you could restore but it will never be ideal it may be difficult be re-placing and grafting the site will put your mind in an easier place.
Peter
Dr. Alex Zavyalov
11/4/2012
What was the initial prosthetic plan? Insertion of only one implant in this area would resolve neither cosmetic nor mastication problem, even though it had been perfectly placed.
Dr way
11/4/2012
The implant was planned for 2 unit bridge , 24 and 25. No surgical stent was used, but initial cone beam was taken .
CRS
11/4/2012
Next time make a vacuform radio graphic stent with barium at the implant site.That way you will have an accurate position for measuring the implant size.Then drill a guide hole for a surgical drill guide. Also when you drill the osteotomy have an assistant stand at the patients feet and help you line up the implant and not pull it towards your side.Taking a cone beam without a stent in place makes it impossible to transfer the position to the mouth. Some cone beams have treatment planning software but you still need a surgical stent lab or computer generated. It's just good treatment planning very simple!
Dr. Alex Zavyalov
11/5/2012
To Dr. way
You’ve meant a cantilever but not a “bridgeâ€, which has at least 3 units
peter Fairbairn
11/5/2012
Youa re right to point that out , what was the plan , i know that economics are important these days but if you are uncomfortable about sinus augmentation ( this should be an easy case ) the maybe 2 implants would work one angled for two teeth the 5 being mad larger to effectively be a 6 .Distal cantilevers in a compromised dentition like this can be testing.
Regards
Peter
Eric
11/6/2012
IMHO you are asking for a lot of trouble and for future failure even if implant was in ideal position with a distal cantilever, especially if it is opposing natural dentition. Mesial cantilevers are more predictable and have a better long-term prognosis.
Maybe you don't have enough bone for an implant to be placed more distally, but I would recommend removing the implant and based upon cone beam, place one more distal and cantilever mesially if possible. If not, remove implant, graft and re-implant after proper healing.
John Highsmith DDS
11/6/2012
I'd take several more films before considering removing the implant. Possible overlap due to angulation, easy to do.
Anand
11/6/2012
Don't think twice , remove implant immediately , fill socket with alloplastic/ resorbable graft material , leave alone for 4-6 months , start again , but this time do a diagnostic wax up using radioopaque teeth or wax ,then take cone beam and a surgical stent/ drill guide to accurately locate the implant/s.
Its hard to say there may just be enough bone to place both 24/ 25 implant.
I won't recommend a 2 unit bridge, with Distal cantilever.
Best lessons are leant the hard way. Good luck
jerry
11/6/2012
If it is asymtomatic and already integrated, I would warn the patient about your concerns and keep it. (You might do more damage to the adjacent tooth to remove it). If it is not integrated, you can try to reverse it out, graft the area. wait a few months and try again.
DSS DDS
11/6/2012
Regardless if a surgical guide is used, get used to taking sequential films. Also, start with small drill, and only to a shallow depth. Keeps even the most experienced and seasoned surgeon out of many problems. For 15 years, I have always drilled and placed a pin in a study model, that is present in the operator at time of placement. Always.
Mike DDS
11/11/2012
Thank you. Great advice. Come beam is amazing, but sequential films are a must. Start with your pilot drill and don't move on till your position is perfect.
Tony Collins
11/6/2012
You have breached 2 rules here.
First - treatment plan BEFORE you place the implant/s - this includes wax-ups guides etc
Second NEVER EVER EVER think about cantilevering off a single implant - all you are doing is creating a level arm.
Keith
11/6/2012
This is the second case posted where the fixture was placed very close to the adjacent teeth. I am concerned with the lack of judgement people are exhibiting. A little preoperative planning like CRS was mentioning could have prevented this. Also, are you taking radiographs during the osteotomy preparation? In addition, it would be nice to think implants do not exhibit crestal bone loss but I ask you this, what if there is bone loss? In addition to compromising the implant, you are affecting the pristine tooth.
Remove the implant and plan the case correctly!
xyz
11/15/2012
well keith its true it will adversely effect adjacent tooth
Theodore Grossman DMD
11/6/2012
After using the surgical guide, confirm the alignment with a film of the 1.0 mm pilot drill. If this is not perfect use a Lindemann drill or re-prep site. Do not compromise the osteotomy.
Gregori Kurtzman, DDS, MA
11/6/2012
Remove it asap its contacting the natural tooth and will cause issues with that tooth. The angulation of the implant does not parallel the natural tooth and a good reason to always take a radiograph after use of the pilot drill to check angulation. also good idea to use a surgical stent. in this case the implant should have been placed further distal maintaining at least 2-3mm between it and the natural tooth
Kevin Mischley
11/6/2012
If the patient is asymptomatic then it is most likely an overlap issue. I can't believe only one other Doc said this. And cantilevering one tooth, especially a lateral incisor off an implant, is absolutely fine. Please remember the rules of crown to root ratio as well as aspects of angulation do not, DO NOT, apply due to the lack of a PDL. I am both a placing as well as restoring dentist and can tell you that an angled abutment will not only allow you to restore this implant but will yield a good and long lasting result. I would leave this implant in and inform patient that is not "ideal". Even say that you could redo the implant but believe it will be fine. I guarantee they will say "we'll, lets give it a shot. It doesn't hurt." And there's nothing wrong with that!
Gregori Kurtzman, DDS, MA
11/6/2012
Lateral incisor cantilver? the implant is at the 1st premolar site and with nothing distal to it cantilevering is a very unwise option
dr.dragos
11/7/2012
Hello!it's about the 24 region,this radiography is not adecvate to appreciate an implant.use an cbct before and after.from my oppinion the angulation and thevcantilever is a problem
geni
11/7/2012
TWO IMPLANTS VERY CLOSED TO EACH OTHER AND WITH SAME ANGULATION WHAT IS THE CHOICE TO LIVE OR TO REMOVE .THEY ARE BOTH WELL INTEGRATED
s.persia
11/7/2012
if patientis asymptomatic i'll leave implant there.you can have a lot of prostetic solutions for restoration.
E.Warde DDS
11/7/2012
Are you joking ?
Refer your patient to an implant specialist to remove this harmful, irrestorable implant and to perform an external sinus lift
s.persia
11/7/2012
of couse I'm not joking, but if there are not symptoms I don't remove the implant ...this is reality and not scientific session...or not. sorry for my intrusion.
Gregori M. Kurtzman, DDS,
11/7/2012
If you look close on the mesial of the implant at the crest there is already bone missing between it and the natural tooth due to its close proximetry. given time this will work apically and lead to loss of the implant and natural tooth. best to remove it now (implant that is) and graft the site and place an implant more distal leaving 3mm between the implant and tooth.
HD
11/7/2012
The film does not look heavily angled to me, only slightly, the contact point between lateral and canine are not greatly overlapped. so i guess the implant-root is very close.
I would take a better radiograph first before deciding however to make sure
I assume the implant was placed angled due to anxiety over the sinus position.
Its better to explain the complication to the patient and deal with it.
SAAD BOJI
11/7/2012
So I think that you need to make better x-ray ,preferably with cone beam .If the tooth canine is asymptomatic so leave the implant ,and try your best to put another implant near by this one ,then to make a bridge of two premolars and a cantilever 1st molar ,my opinion that there is enough bone to put another implant !!!!!!!!.in the next time when you are going to put implant ,always you should take an x-ray simple one,after the first drilling with 2.0 mm drill to see the pathway of drilling and the expected site of implant then continue to fix the implant !!!!!!
Gregori M. Kurtzman, DDS,
11/7/2012
Distal cantilever a molar? Please show any lit that shows that being successful or recommended. A distal cantilever molar has always been frowned up due to high occlusal loads placed on these leading to failure.
ttmillerjr
11/9/2012
There is risk leaving this implant in place. Just take it out and do it correctly.
salim hazim
11/9/2012
If the implant invaded the periodontal ligament the colleague will not post this case and wait our advices. About the angulations it is not only inclined mesiodistaly but it is inclined buccopalataly and it is inclined palataly because the labial plat is too thin to insert an implant labial to the canine in such a manner , so the abutment of the implant is severely inclined labialy. So implant with severely inclination in two plane and platform in a level about few mm under the level of cementoenamel junction of the adjacent tooth in addition to esthetic problems with severely inclined abutment labialy in a severely apical level what kind of prosthesis will be result and about what kind of cantilever we are talking about, let us not forget the effect of few mm of angulations on the crestal bone resorption imagine this with this complicated angulations and cantilevering.
DrT
11/9/2012
There are 2 main issues here (and a few secondary ones such as the use of cantilevers which is best left for another discussion):
1. Will this implant, once it is restored, have a predictably good long term prognosis?
2. Is the adjacent canine being compromised in any way?
My answer to these questions are: NO, this implant, even if it could be restored, will have a poor long term prognosis because of the bone loss that is already evident mesially, and also because the eventual direction of occlusal forces will most certainly not be along the long axis of the implant; second, the canine is already showing involvement of its bone on the distal, and additional bone loss on this surface is inevitable.
I think in cases such as this (and we have ALL definitely had them), the question that we ought to be asking ourselves is not what COULD we do, but rather what SHOULD we do. We have all deviated from the ideal, not only in implant dentistry but most likely in our practice of general dentistry or in our speciality. IMHO, we need to try to keep these instances to a minimum, and each and every time we do this, we ought to ask ourselves if this is what we would want in OUR mouth. Thank you.
DrT
CRS
11/9/2012
One thought since I'm a specialist who does not restore, there is a second pair of eyes keeping me honest. I want the best possible implant placement not only for the patient but for the referring/restoring dds. i don't want to create a headache for him or our patient.. I like the team approach it's mutually beneficial!
Gregori Kurtzman, DDS, MA
11/9/2012
This case is a good example of lack of proper planning. a surgical stent shiuld have been used to ideally place the coronal aspect where a tooth would be which means in this case leaving a minimum of 2mm (preferable in this case 3mm) of space between the implant and natural tooth. We can then debate angulations which may be needed due to angulation of the bone but typically in a premolar site the implant can be placed more vertical which as Dr. T pointed out loads the fixture better. also in this case we have to ask what is the prosthetic plan to replace the missing teeth in that quadrant? Will this implant be restored with an attachment for a partial or a crown to clasp with a partial?
Dr G
11/13/2012
I wouldn't want that in my mouth. Why such poor planing? If you can't do a lat. wall sinus lift then honestly you just should stick with the basic cases.
1. No educated surgeon/dentist would treatment plan a distal cantilever premolar.
2. No experienced surgeon would create this type of situation.
Where is your conscience?
s.persia
11/16/2012
dear colleagues who never ever makes a mistake, blessed is he who among us has never failed ... here there is a problem but I think that few are sincere at all and I still think that most of us would leave the implant where it is asymptomatic right now.
Dr.S.Lin
11/19/2012
To remove it, you better do it within the first three weeks. Once the implant is well integrated, you wont be able to torque it out. A trephine of a slightly larger diameter than the implant will have to be used. In such instance ,you will surely run a great risk of damaging the adjacent tooth even in an expereinced hand.Take a ct , it's an acurate way of determining exactly how close it is, PAx could be misleading.
This implant maybe just fine if symptom does not arise. As far as crestal bone resorption on the distal of Canine, if the pateint has a thick gingiva biotype, chances are low .
Live, love, and Learn !

















{kind=link}
{kind=link}