Massive lost of soft tissue after implant placement: recommendations?
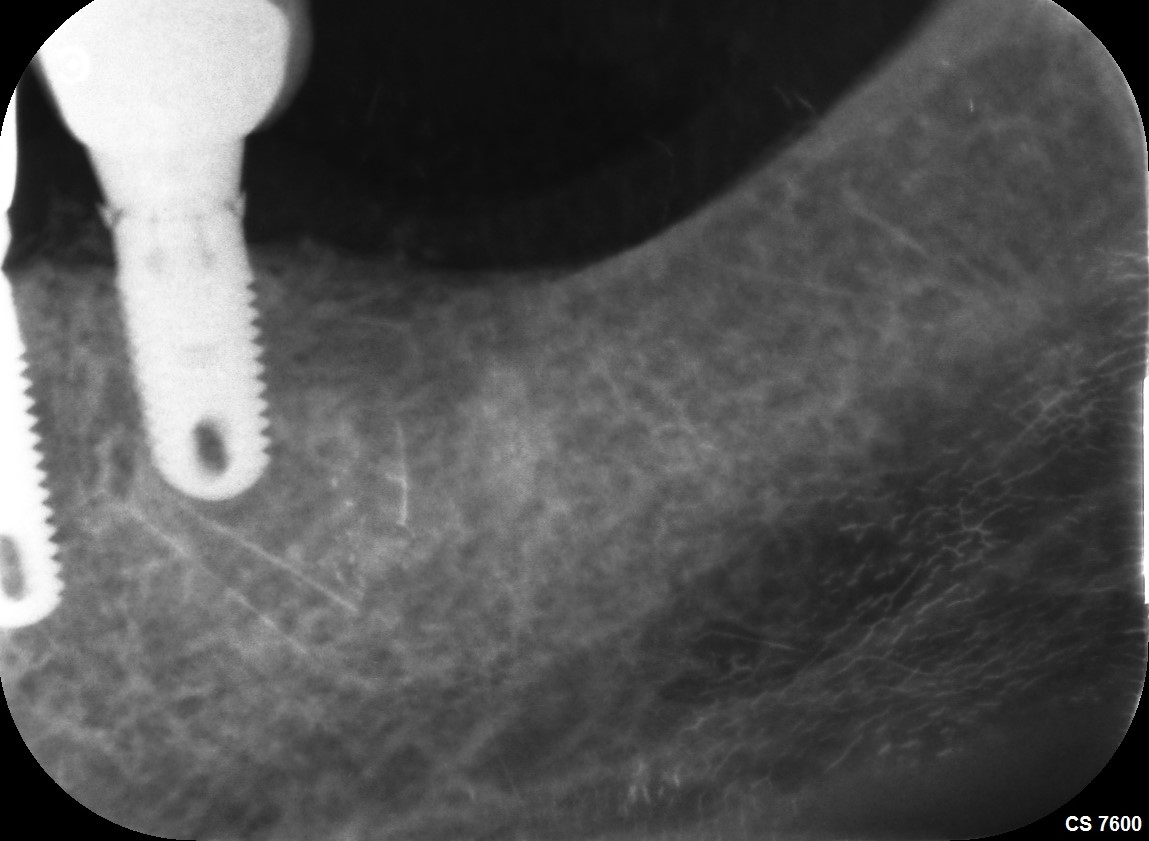
I was referred a patient to do an implant crown on site #9 [maxillary left central incisor;21]. The implant was placed at the time of extraction and a guided bone regeneration procedure was also performed. This was done by a periodontist.  As you can see from the clinical photograph the patient has suffered massive soft and hard tissue loss at that site. I do not see how I can possibly restore the case and achieve an acceptable aesthetic result. Do you have any recommendations how I can proceed?
(click image to enlarge)
45 Comments on Massive lost of soft tissue after implant placement: recommendations?
New comments are currently closed for this post.
CRS
1/26/2013
It would be very helpful to have a pre and post op film. I suspect that the hard and soft tissue defects were not addressed at the time of implant placement. We're you involved in the initial treatment plan? Placing an implant in the exact same site as a periodontally involved tooth usually will not regenerate all the lost tissue. Proper site preparation in the esthetic and functional zones is key. Immediate placement at extraction works if you have an ideal, healthy site with a thick biotype. I suspect that the implant may be too close to the natural tooth and possibly too large, there is no intradental papilla. I can't see thru the tissue! Anyway this is not your problem the operating periodontist needs to refer a restorable implant. What does he say? I would definitely say that the case is not ready to be restored needs to be discussed so that you will not be holding the bag if the implant fails. Pink porcelain is not a sin but it needs to be treatment planned as an option. Good luck I always feel better with a team approach, you needed to be involved at the get go with the periodontist.
pon
1/27/2013
Thank you so much for your comment. Actually this tooth was extracted due to endodontical failure with bone resorption. I did discuss with periodontist before and insisted not to do immediate placement but she thought it could be done with bone and soft tissue graft. Anyway it's too late to complain. Sorry that I didn't attach radiography after surgery, the implant is right in the middle , not close to natural teeth. Anyhow, I feel sorry to this patient so I have to try to do but will tell patient for not expecting high esthetics result.
Any comments or suggestions would be helpful and appreciated , Thanks
CRS
1/27/2013
Find a new periodontist who understands site development. I'm sorry that this happened it probably needs to be redone with proper grafting and staging. This will need to be handled carefully without playing the blame game. I suggest you have the periodontist handle this result and refer appropriately. Now here is how I would fix, I would remove the implant and extract the lateral also and do a guided PRGF, allograft with a membrane, use an Essex to keep pressure off the graft. The contralateral lateral needs a CT graft also. Your canines look good . That way you can match the anterior teeth. Also how is the occlusion and perio of those lower teeth. If this is going to be a headache I would refer to a trusted prostodontist you'll sleep better. The specialist needed to listen to you as a team member, ie quarterback! Best wishes.
dbe
1/29/2013
the lateral dictates horizontal bone height so it is shot. remove, needs hard and soft tissue reconstruction and single implant at 9 with screw retained 2unit bridge is it. good luck, hard to hit home run everytime. poor treatment planning by surgeon.
Peter Fairbairn
1/27/2013
Even without X-ray you can see this Implant has been placed deeply.
This will be difficult to remedy , refer back to the placer as he would not be happy with this result either .
Peter
Pynadath
1/27/2013
Implant head looks at good level but obviously loss of bone and soft tissue. Was the bone graft placed at time of the immediate placement lost or was there loss of the buccal bone plate?
pon
1/27/2013
Thank you so much for all your comments and suggestions. I will discuss with the patient and talk to the periodontist
Richard Hughes, DDS, FAAI
1/28/2013
I suggest that you step back and look at the whole mouth. This patient is a Bruner and has some orthodox/perio issues. I agree, remove the implant. Then graft with dense HA and make a simple and aesthetic six unit FPD from 6 to 11. You will save the patient a lot of time and money and you will not have as many head aches. Goog luck.
CRS
1/28/2013
Excellent idea.Especially since grafting in this compromised area may not be ideal. I like to see how the grafts heal prior to any implant placement. I would still remove #10 based on the tissue loss but need to see a film, possibly salvageable. The graft with restoration of the lost buccal bone will aid in the long tem prognosis of the bridge. The fixed bridge s a great option after graft healing. Great option again Dr Hughes!
Dr. Alex Zavyalov
1/28/2013
If the implant integrated well, I would proceed. The defect may be easily corrected with pink porcelain, but nobody can say that after extracting the implant, grafting or moreover, extracting the adjacent lateral incisor, the situation will become definitely cosmetically better.
Peter Fairbairn
1/28/2013
The only reason why I mentioned the level which we cannot truely see as no radiograph as asuming what we see is the healing cap it would denote deeper placement. Which is fine with bone present but with the loss of bone between the implant and the lateral having led to the loss of soft tissue it becomes more complex . Here you would need the Implant less deep to able to restore the bone with graft material .
No bone no long term solution.
Peter
Dave Robinson
1/28/2013
I wonder if it is worth trying a zirconium abutment with porcelain crown . Possibly try a temporary crown . See where the gum ends up . Just doodling here but is that a healing cap , or is the implant head partially exposed and that is a cover screw? Dave
KPM, DMD
1/29/2013
I'd say if that implant is solid and integrated, then leave it alone! That is, don't remove it. Speak openly with your patient about the challenges that you are BOTH facing and give the options of going ahead and restoring (with pink porcelain, etc) vs. drilling that thing out and going through months of surgeries AGAIN. I bet the patient would like to give the first one a shot. This is an extensive defect. What kind of result can we hope to predictably achieve by removing the solid implant, grafting the area for hard tissue regeneration and then perform what is surely going to be multiple soft tissue augmentations? At worst, you do not achieve the already anticipated compromised esthetic situation and, in the grand scheme of things, you do not waste THAT much money. At this point your patient will probably appreciate your trying to work with what she has. Then again, only you know this patient's mood. That surely factors into your decision.
Mark P. Miller, DDS
1/29/2013
As usual, Richard Hughes is spot on. Are you and the patient happy with the implant? With #7? With a long #8? With a very compromised #10? Look at the near perfect symmetry of #6 and #11. I, too, feel that the best solution is a six-unit anterior bridge. The patient needs to know at this point that any solution involving #9 alone is probably a poor option esthetically. If the four anteriors are removed, a reinforced 6-unit temporary bridge can be placed. The patient would have immediate teeth, healing could take place in a controlled fashion, and esthetics can be controlled with pontic design. Pink porcelain is the only answer if you choose to treat just #9. But it strikes me as trying to place a new wheelhouse on the Titanic. Also...in hindsight...the implant should have been placed following healing of #9 site. Just because we CAN do something does not mean that we SHOULD do it. Good luck.
Dr. Steve
1/29/2013
Obviously, an accurate diagnosis is warranted and I would not be interested so much in x-rays as much as a CT Scan. This should be the start of your plan and a mistake would have been made to implant this patient without one.
Peter Hunt
1/29/2013
There is not really enough information to know if the implant is malpositioned or if the implant platform is too large/small. What is obvious is that there is massive tissue loss between the implant and the lateral incisor. Removing the lateral incisor at this stage would only accentuate the problem.
The optimal way to manage the situation now would be to erupt the lateral to bring the hard and soft tissue complex on the mesial crestally. How much? Sufficiently that the mesial papilla on the lateral incisor "balances" that on the contra-lateral side. This in turn would allow the lateral incisor to be removed and a second implant placed, and for the soft and hard tissue complexes in the region to be properly re-aligned.
steve c
1/29/2013
Assuming the implant is well positioned and the bone levels are good, you could place a connective tissue or a palatal pedicle graft over the top of the ridge and the implant. It would require that the healing abutment be removed and replaced with a coverscrew. This procedure would cover the implant entirely and after sufficient healing and maturation, the implant could be uncovered and a healing abutment placed again. If needed this is another opportunity to place more palatal gingiva or potentially even a soft tissue allograft if appropriate.
Removal of a well integrated implant together with ridge augmentation and possibly gingival grafting is certainly another option, but it is highly invasive and there is plenty of room for a poor outcome unless the surgeon is highly skilled.
Pankaj Narkhede DDS MDS F
1/29/2013
I think you should send him back to the periodontist. retreatment required. The patient needs occlusal equilibration etc
DrT
1/29/2013
I agree with Dr. Hunt. Unless you can improve on the height of the alveolar bone on the mesial of tooth #10 I cannot see where any acceptable esthetic result can be accomplished (except with pink porcelain but this will be of questionable esthetics and oral hygiene will be compromised). I also would not proceed too quickly to fabricating a six unit FPD if you are dealing with two virgin cuspids. Forece eruption followed by removal of tooth #10 and then site development of the area of teeth #9 and #10 is the way I would proceed.
DrT
Carlos Boudet DDS
1/29/2013
You can see many red flags in this case that the periodontist should have been aware of.
Thin Biotype
scalloped tissue
tapered teeth
I do not know where the tissue was before, but I assume that the destruction of interproximal bone and interdental papilla between the central and the lateral is iatrogenic in nature.
Trying to reconstruct the normal architecture now will be very difficult and demanding, and will require both hard and soft tissue grafting.
Restoring this case as it is now will be dissappointing both for you and your patient.
Carlos Boudet DDS
1/29/2013
I have tried forced eruption in a similar case, and it is not enough.
You will still need to do bone and soft tissue grafting or the bone will dissappear after you sacrifice the lateral and place the implant.
Good luck!
DrT
1/29/2013
May I suggest that we refer to the surgeon in this case as just this,,,the surgeon. It feels like continuing to interject that a periodontist placed the implant in this case is introducing a polarizing issue that currently exists in implant dentistry today re who should be placing implants, and this takes away from all of us trying to objectively help the poster of this case. Thank you.
DrT
Dr G
1/29/2013
Initially I was a little freaked out by this picture, but if you look carefully there are a couple of positives. 1. Something made this defect post surgically based on the inflammation in the area. 2. There is a palatal I/P papillae. 3. Tooth #10 has a decent attachment apparatus. With all of this info I'd do the following. Create a beautiful temp with a broad contact point between 9/10. Leave it alone for 3 months. The papillae should start to return with adequate Oral hygiene. The periodontist could assist this process by coronally repositioning the buccal flap at this 3 month point. This again would improve the appearance. The one thing I would stress is the temp must be pristine, polished, cement free and the abutment must have a great, not good emergence profile. Patience will win in this case.
DrT
1/29/2013
Without any bony scaffold on the mesial of tooth #10 I cannot see how you expect any coronally positioned gingiva on the buccal to be maintained, even with some residual palatla papilla, In addition, if per chance you do get some more gingiva buccally what you are in essence doing is creating a supra bony pocket on tooth #10...good luck maintaining that in the long term.
DrT
Dr G John Berne
1/29/2013
My first comments are that this a perfect example of why implants should be placed by the person doing the final restoration. That way you fully appreciate the problems of poor implant placement in relationship to the final restoration. This case also shows why immediate implant placement is frequently not the best option and should be done only under ideal circumstances. There is a lot of research showing that the result from immediate placement is often inferior to a 2 staged approach, particularly if the alvoelar bone at the crestal margins is thin.
Having said that, it looks like bone and tissue grafting are the only realistic options for this case if the esthetic demands are overwhelming. Fortunately the gingiva doesn't appear to be a thin biotype so there should be a realistic chance of reasonable improvement with grafting procedures.
dbe
1/29/2013
i disagree. a surgeon should operate and the dentist do dentistry. the extra details after20 years operating cannot be picked up placing minimal implants.
Dr G John Berne
1/29/2013
You're absolutely right about the benefits of having 20 years of experience. Unfortunately the only way of getting 20 years of experience, regardless of who does the surgery, is to place implants for 20 years. So everyone has to start somewhere. The important thing is that you stagger your cases, starting with the simple cases then as you become more proficient, move on to more challenging cases. But regardless of experience at placing implants, if you don't understand the prosthetic requirements of implant placement, then you will continue ending up with results like this. After all, implants are fundamentally prosthetic driven and a thorough understanding of the prosthetic requirements is mandatory for implant placement.
CRS
2/1/2013
It was not the prosthetic needs of the case but the restoration of the alveolar bone to support the implant. I have seen with failed endodontic teeth, compromise of the buccal plate, fenestrations and retrograde bacteria . It was a compromised site at the get go. Staging would have been appropriate to see what result was obtained prior to implant placement. An implant is inert, prevents the blood supply reaching the entire socket it can however be a scaffold for bone growth. The prosthetic requirements in my hands can be obtained with a well made surgical stent made by the restoring dds and if he tells me what he wants I can obtain it for him with a team approach and good communication. I always welcome the dds to attend the surgery and they learn my world, and they tell me what they need. It is very satisfying to work as a team especially when you have a challenging case nd be able to recognize it. You can't do everything well but need to use what you do best for the patient. A doctor should try for nothing less and not let ego,money and turf battles cloud their judgement . This case was handled poorly by the operating doctor ho did not listen to his/her referring dds. Please take me with a grain of salt, no X-ray, and I was not present at the surgery. Thanks for reading!
Dr. Omar Olalde
1/29/2013
1. What are the expectations of the patient.
2. What about the line of smile, how much teeth he shows when he smile?
3. Remember the biological width, the bone is 2-3 mm below the soft tissue.
4. A prostheses sometimes replace teeth and some times teeth and soft tissue.
If the implant was placed by a Perio with minimal experience in dental implants, much probably the lack of bone in the papillae area was already there.
How shoul I proceed, tell the patient the point 4. You will have the ideal result only if you have the ideal case.
Please add an Xray, I can't identify if it's the cover screw or the healing screw.
If it is the healing screw you have some chances to improve aesthetics. I'll write how.
Dr. Omar Olalde
1/29/2013
Paying attention to the picture, did someone used an electroscalpel to uncover the implant?
Dr G
1/29/2013
Experience counts in this case. An earlier poster suggested an onlay graft, CT graft ridge augmentation. This as well is a great suggestion. Under perfect conditions things happen. I've seen loose flippers destroy healing buccal contours. Dr T this is a case for experienced experts. Think it through, does a CT graft attach to the facial of a tooth with recession? It's unfortunate this case happened, but I would be the last to cast blame. Most people have good intentions. What we need to use this medium for is solving the problem presented not speaking from the soapbox. This is a "grey zone" case. There are multiple solutions all are not perfect.
dr gerald rudick
1/29/2013
Unfortunately there are no radiographs presented; however by the photograph supplied it is evident that this patient has an orthodontic problem that might have originated from tongue thrusting. The lower incisors are fanned out and the left upper lateral ( #22) is covering the lower incisors but most probably has limited bone supporting it and hence the loss of the soft tissue.
Removing the implant is a good option if it can be done atraumatically....followed by bone building via a bone block or titanium frame; orthodontic distraction should be considered for the upper lateral in order to drag it down as much bone as possible before extracting it......is the patient a smoker?????? none of this will work if smoking is a factor.
This is not a simple case, and the patient must realize that it might not come out the way he/she wanted it...another option might end up being a partial denture replacing the central and lateral, and using the present implant as a possible retainer for it......not an easy situation to remedy.....
Dr. Michael Cangemi
1/29/2013
Let's consider looking at the larger picture: Why was #9 lost, why is #7 crowned?. Look at the flaring and spacing of the maxillary and mandibular anterior teeth. The generalized abfractions (restored and non-restored). What appears to be a cross-bite of #12 (certainly rotated). The poor occlusion on #5, possibly missing #30. Pocket issues (NOT just #9 site and #10). Mobility issues? Proper and adequate cuspid guidance that can override the probable generalized bilateral interferences? If one wanted to super-erupt #10, are there adequate stable anchors. Is there a tongue thrust or other habits? I just think a much more detailed analysis of the occlusal scheme is warranted before jumpint into a bridge and some of the other options put forth in this forum.
Just saying...
Harry Karna DDS
1/29/2013
U hit the nail on the head. The occlusion is not analyzed in this case at all. The patient probably has a CR-MIP slide resulting in too much lateral force with no centric stops in the back compounded with periodontal problems. There is a high probability that the anterior flaring is due to the CR-MIP slide. U can also observe that the plane of occlusion is not proper hence creating premature contacts to complicate this problem. This looks more like a full mouth rehab with a proper planning for an acceptable occlusal scheme.
This case needs a FM photos, FMX and mounted models in CR to do the proper planning.
I get a feeling that even if we were to get some kind of acceptable restoration on this, we will still have long term problems of stability due to perio and occlusion not being addressed.
Michael H Cangemi
1/29/2013
I agree Dr. Karna...
Thanks for the additional points to consider...
Mike
greg steiner
1/29/2013
I don't think this is as bad as it looks. It appears the only tissue lost is the mesial buccal tissue on tooth #10. The esthetics of this case was a disaster before implant placement. I would conclude with Dr. G and place a temp as he described and let the body resolve much of this defect before attempting any further regenerative therapy. Also the patient did not care much about esthetics before treatment and he may not be concerned now especially if there is a low lip line. Greg Steiner Steiner Laboratories
Peter Fairbairn
1/30/2013
Having recently spoken at a prominent University , it was interesting to see that still the concensus of Perio acedemia is that occlusion and or parafunctions do not cause bone loss according to the evidence .
Such is life.
But this case will only be resolved to the patients and the dentists satisfaction with hard tissue regeneration thus an x-ray would be helpful.
Peter
Richard Hughes, DDS, FAAI
1/30/2013
Dr Berne, great advice. You have to crawl before you walk. I started off with simple cases and worked up.
Alan Jeroff
1/30/2013
If you are going to remove the implant , I would suggest that you use the Neo Fixture Remover Kit. It removes the implants atraumatically. I used it on a case where the implant had integrated for 3 months and it just unscrewed. Good Luck.
CRS
1/30/2013
Okay, I think that the "implant googles"were on when this case was treated. Look at the whole patient, occlusion, esthetics,bite collapse, failed endodontic. Instead of rushing to extract,graft and place an implant site preparation first. Let things heal then place the implant. This case gives specialists a bad name. Just because an article us published with immediate placement doesn't mean it should be done in every case. That said we all have had poor outcomes myself humbly included. Now there are two paths, revision,repair or restoration with pink porcelain. Trying to orthodontic ally erupt th lateral will just exfoliate it, that technique is used for worn down teeth with decent bone around the root to bring the alveolus with it. Removal of the implant may give you an even bigger hole to fix don't have a film to evaluate. What does the patient want? A low lip line and good oral hygiene may save you. I would advise the patient that over time the implant and lateral may fail and a revision of the treatment may be necessary. If the patient is happy with the provisional, go from there. We are all trying to predict the future here. My first rule is do no harm to the patient, but the ideal result has not been achieved so you go from there. I think it is a shame if a restoring dds thinks that they can do everything well, I know I can't. A team approach is best and that was not done here, the dds is holding the bag due to what I feel is a poor treatment decision by a specialist, it happens. You don't know what you don't know. There is no substitute for experience and training some folks have to learn the hard way. It's what you do with a failure not judging that counts. I find this forum very stimulating n beneficial. I would really enjoy working with. A lot of these fine posters. I would love to see how this case was finally managed! An yes I started out 20 years ago there was not alot of implant training or systems or pushy salesmen or weekend courses. I proceeded very carefully using the skill gained from placing bone plates in the OR and grafting bone from the iliac crest it was my core competency and built on that . I knew that restoration was in the hands of the dds who does this with greater skill than I and rely on a good treatment plan and surgical stent. We are here to help each other! Do want you do best an build on that thanks for reading!
Dr Kimsey
1/30/2013
Forget who placed it or who should place it the problem is what to do now. I would remove the implant and take time to build what I could and then place it again.
Edoardo Calvi
1/30/2013
Umfortunately there is no way you can fix it without invasive surgery. For sure at the time of the first surgery there was a massive bone lost around the lateral incisor, when the periodontist cut the gum the soft tissue collapsed. There is only one solution: extract the implant the lateral incisor, let the tissue heal for 12 weeks and make a vertical ridge aumentation with a reinforced gore membrane. After 8-9 months take out the membrane and make a CT graft. Let it heal for a while and decide if make a bridge that goes from the incisor to the canine or place two implant ( flapless ). The bridge is easier to handle. For the vertical augmentation you have to extract the lateral incisor because you need the peak bone mesial to the canine. It is difficult but a very good surgeon could it.
I hope i was clear enough. Sorry for my poor written english.
Edoardo
Edoardo Calvi
1/30/2013
One last thing, if the patient has a low smile line just restore it.
Maximiliano Hespanhol
1/31/2013
Are you familiarized with L-PRF (platelet rich fibrin) membranes; If so, you could try it out. If not, take a look at Professor Choukrouns mehod using it.
All the best.
Paolo Rossetti - Milano
2/1/2013
Hasn't anyone considered the orthodontic extrusion of the lateral incisor?
I mean in case the rough surface of the implant is in the bone.