Necrosis of Gum with Bone Exposure: How to Manage?
My patient is a 60 year-old male with controlled diabetes, smoker (15 sticks a day). On 12/14/19, I surgically installed 3-implants in the lower right quadrant with bone augmentation consisting of mostly autograft collected during the drilling. A Jason membrane was placed over the graft and the flap was closed with Vicryl sutures without any tension. An antibiotic was given 2 days prior to surgery as pre-operative medicine and continued for 7 days. Chlorhexidine with hyaluronic acid mouthwash and Gengigel were prescribed after surgery.
2 days post-op (12/16/19), the patient called complaining of a little pain. I told him this was normal and to take Diclofenac. At 5 days post-op (12/19/19), the patient called complaining of too much pain. When I checked the implant site, the gum was open, the Vicryl suture was still in place and the suture was lose but not lost. There was a bit of gum necrosis. I cleaned the wound with saline irrigation and placed silk suture. I instructed the patient to avoid smoking and patient agreed. After 3 day follow up (12/22/19), the area of gum necrosis became larger and the silk suture was still in place. I made a stent of soft material to cover the wound and the necrotic area. I instructed the patient to put hyaluronic acid under the sent. After 3 days follow up (12/25/19) there is no improvement and it became worse. I prescribed Vitamin C. How can I manage this? I don’t know.
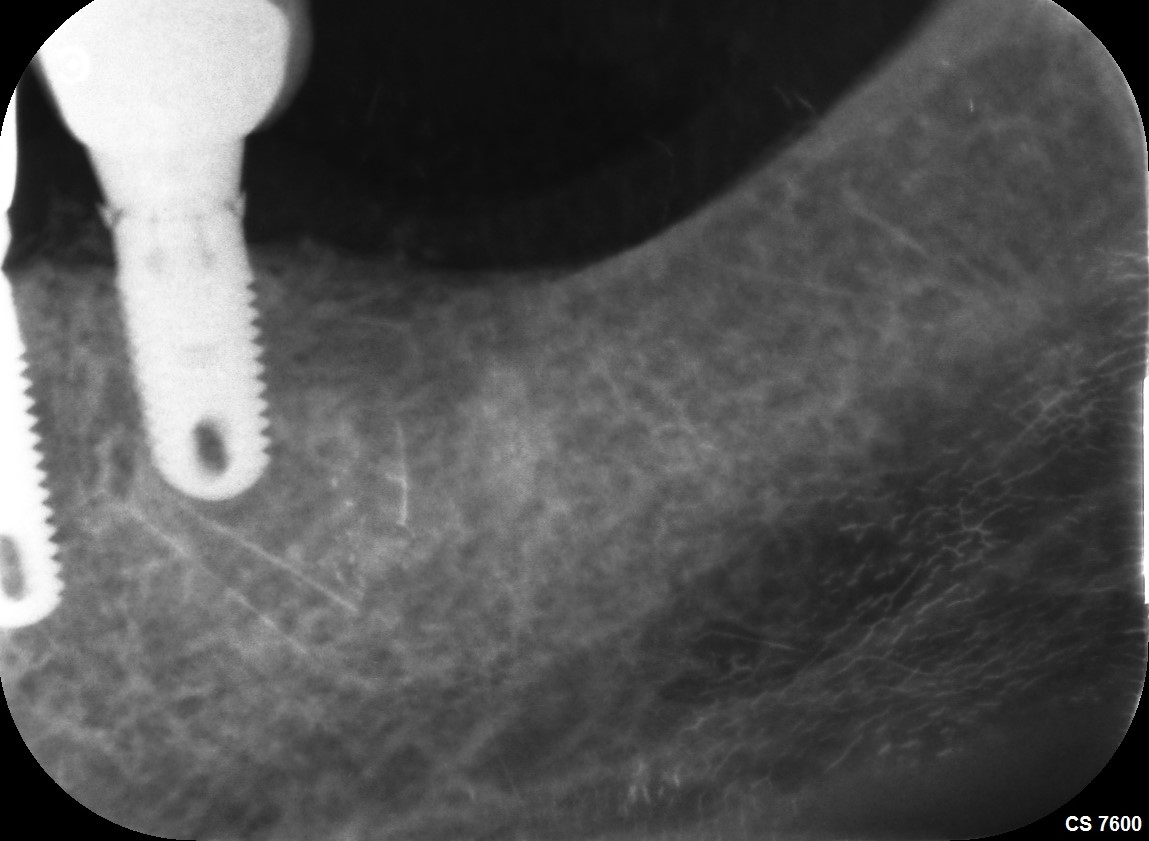
![]5 Days Post Implant](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/12/20148-24-panorama5-days-status-post-implant-e089f2f9d687.jpg)5 Days Post Implant
![]7 days after surgery](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/12/20148-24-photo-taken-7-days-after-surgery-e089f2f9d687.jpg)7 days after surgery
![]12 days](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/12/20148-24-photo-taken-12-days-after-surgery-2-e089f2f9d687.jpg)12 days















5){kind=link}
7){kind=link}
12){kind=link}