Bone Graft with Implant Placement: What option do you recommend?
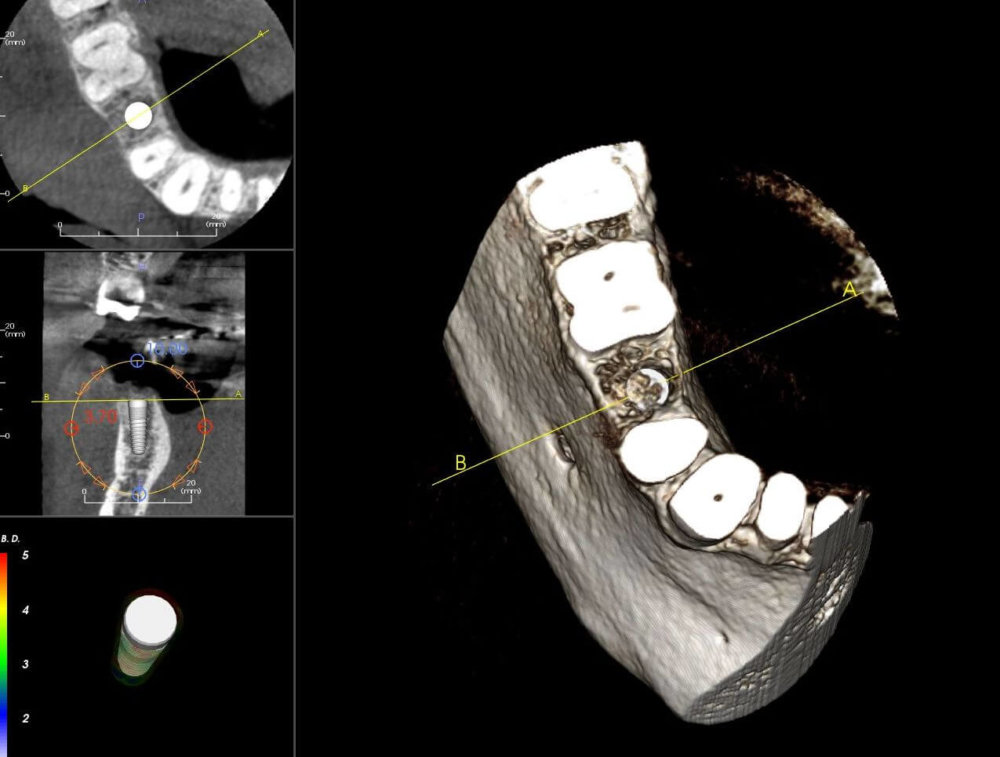
This graft at site #29 has been in place for 6 months. The bone is generally good except for some gaps notably around the lingual aspect. Both lateral plates are intact.
Here are the Options: 1) placing implant as is 2) placing implant with bone graft to fill gaps 3) redo graft and wait.
What option do you recommend?
![]Bone Graft with Implant Placement](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2018/10/8162-24-1-bb56c1c424b8-e1538658077386.jpg)
![]bone is generally good except for some gaps notably around the lingual aspect.](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2018/10/8162-24-2-bb56c1c424b8-e1538658030493.jpg)
5 Comments on Bone Graft with Implant Placement: What option do you recommend?
New comments are currently closed for this post.
Timothy C Carter
10/4/2018
A titanium screw. It doesn't have to be any more difficult than that. In my office it would be a Zimmer TSV but that is just the brand I prefer.
Osurg
10/4/2018
Place implant any system you are comfortable with. Just be aware of length since you are above nerve.
Timothy Hacker DDS FAAID
10/4/2018
The first and second mandibular premolars provide some challenges. The most predictable approach is to graft the socket, wait 4 months and place your implant. It's so much easier to have a conversation with the patient about the challenges and why you are conservative before you have problems with the implant and/or nerve and have to bail out.
Sdddds
10/4/2018
I think you are good to go with implant placement as is. I would use a longer implant than the projected one you show as you have plenty of bone height. The width looks good. I commonly will add a little graft material on the buccal when there is a small defect (or a larger one) as shown on the CT scan here.
BJP DDS DICOI
10/4/2018
Question is. Have you bone sounded the area? If the grafting has been compromised with the migration of fibrous tissue you may not have primary stability upon placing the implant. A 4.0 (3.7) x 12mm implant size is ideal for that space as long as you don't violate the 1.5 -2.0 mm distance from the adjacent teeth as well as compromising the integrity of the IAN. I would prepare to place the implant, worn the patient ahead of time and include it in the informed consent that the bone may have not matured enough as planned, and if you encounter any fibrous tissue infiltration at the time of exposure of the implant site, stop, remove the immature graft, curette thoroughly and re graft the area and allow another 4-5 months to heal.
If the bone is well vascularized and you do not encounter any fibrous tissue in growth, create the osteotomy, place the implant and if you see a need for it, graft the crestal area of the implant with bone grafting and or sink the implant 1.2mm sub crestal achieving primary closure. Current research shows that unlike a tooth with a PDL, an implant sustains the greatest amount of stress at the crestal 4-5 mm's not down the long axis of the implant as a tooth does with a natural PDL.


















{kind=link}
{kind=link}