Platelet rich fibrin as a graft for crestal bone loss?
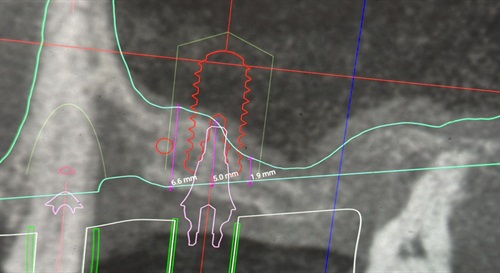
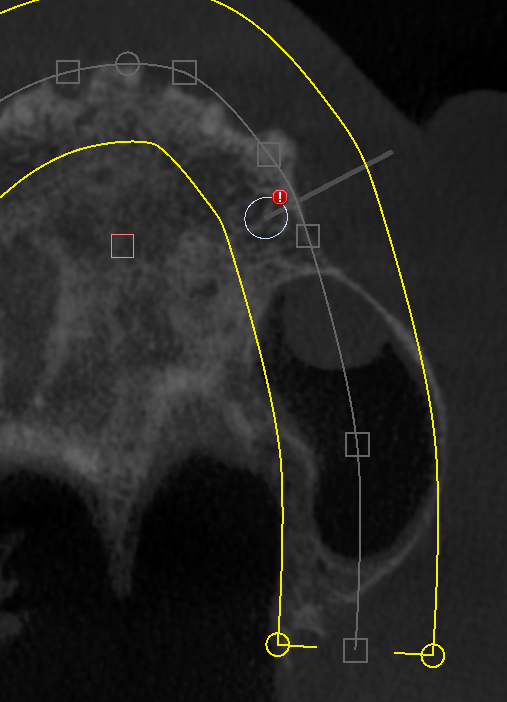
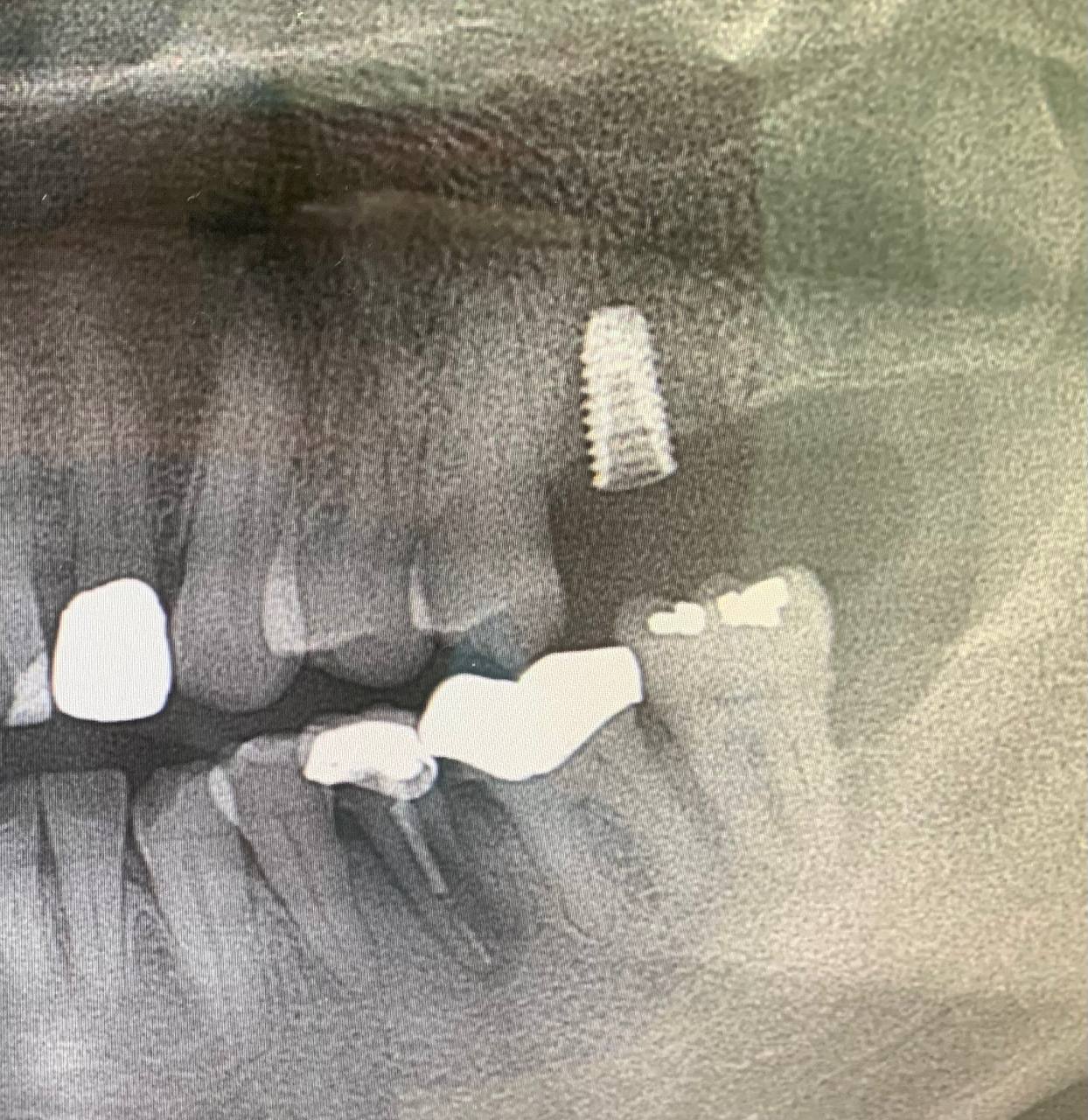
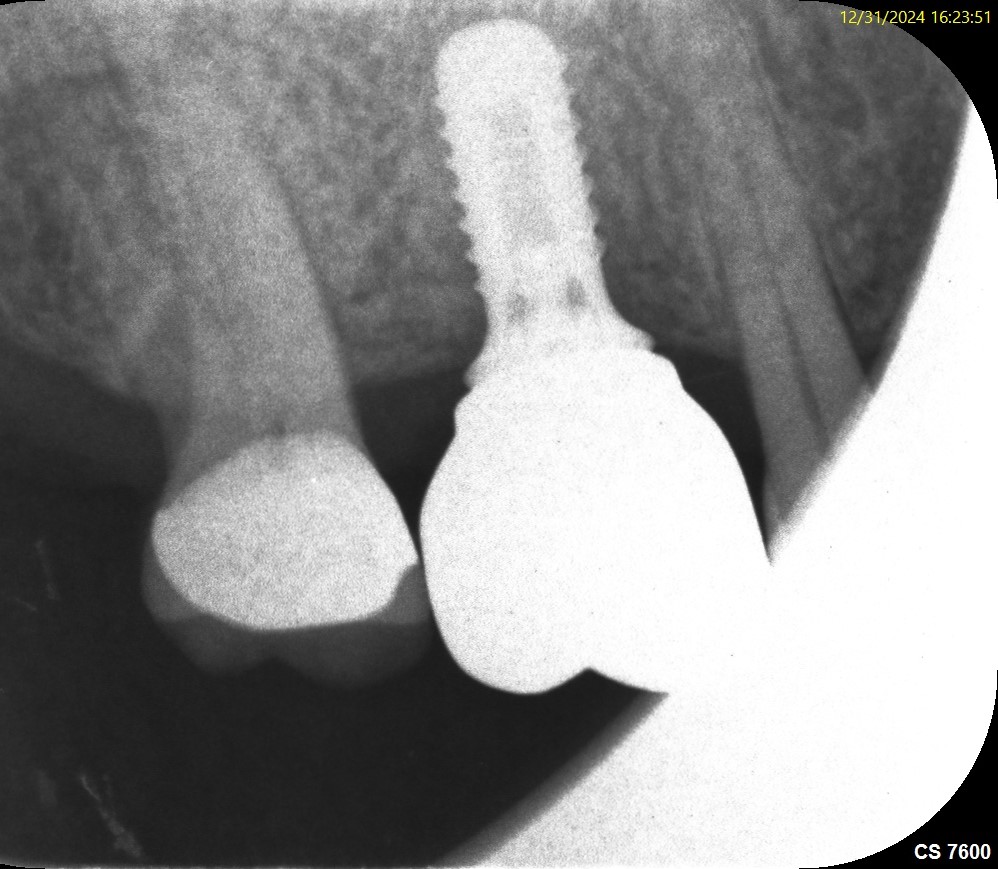
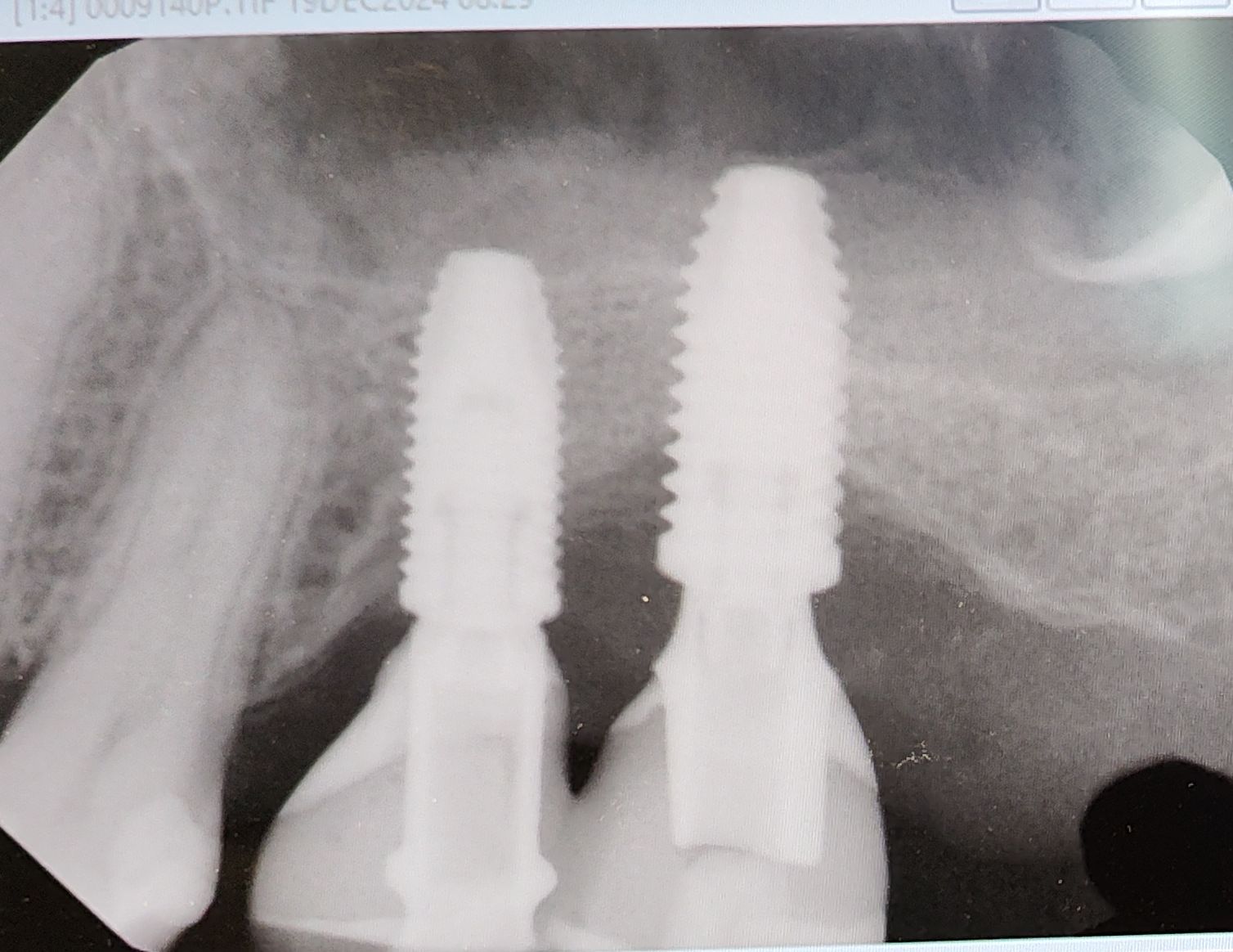
I have a case with early crestal bone loss. The implant is exposed below the first thread after 3 months of insertion, even without loading. Can I use PRF [Platelet Rich Fibrin] with a bone graft to cover the exposed thread for this implant to survive? What are the other options for covering the exposed thread?
8 Comments on Platelet rich fibrin as a graft for crestal bone loss?
New comments are currently closed for this post.
Robert J. Miller
2/23/2014
The quick answer is yes. But unless you understand why the bone loss occurred initially, you may not have success in regeneration. Is it related to implant architecture or higher microleakage abutment connection? If so, no graft material, including PRF, will regenerate this tissue. Is it from a lack of keratinized tissue or a mobile mucogingival junction? Regenerate the tissue first and then regraft. Is it a pathogen mediated peri-implantitis? If you can surgically clean the implant surface, regeneration that includes PRF has a good chance. Is it generalized horizontal bone loss with the threaded portion above crest? Vertical bone augmentation with a biomaterial mixed with growth factors is your best bet. PRF alone will not regenerate the height you need. Is it an infra-bony defect? PRF alone, with primary closure is a good strategy. If the threads are above the tissue and you cannot get closure over the implant, an implantoplasty is your best choice.
RJM
mark
2/24/2014
Beautifully said Dr.miller.can you please highlight the procedure of obtaining prf?
CRS
2/24/2014
Very good treatise, but is think the post says that this implant is not loaded so there could not be abutment issues. My question is was this an endodonticaly treated tooth with bacterial issues? Is the patient wearing some kind if flipper traumatizing the tissue or causing movement? Was there primary stability at placement? Without a film and at this early juncture I would open it, clean it raise a flap with release to primary close it and place bone with fibrin or a resorbable membrane. I think it has to be fixed now prior to loading or you'll be chasing it in the future. I think it is bacterial problem. I hope this helps!
Robert J. Miller
2/25/2014
A discussion on how to harvest PRF and use it clinically would be too lengthy for this forum. Best to go to the PRF portal at intra-lock.com for a good synopsis of the procedure and some technique videos.
RJM
Joseph CHOUKROUN
2/25/2014
Early exposure of the implant is coming first from a soft tissue loss.
May be your implant is too crestal ? Or suture without tension free flap closure ?
With these errors, PRF cannot help you.
If you want to do a graft: 1. what kind of biomaterial will you use ? Allograft is the best 2. Pure Metronidazole added to the graft is a good opportunity to protect the graft material from the contamination. 20-50mg mixed with the granules 3. PRF should help you in this protocol.
Dr. Gerald Rudick
2/25/2014
You must look at the neighborhood this implant is "living in"........are the natural teeth around it pathogen free.....or is there a sea of bacteria and toxins in the immediate area? You must make sure there is no periodontitis affecting the local teeth .
PRF is an excellent solution to providing growth factors to a region where you want to enhance the bone....but as Robert Miller states, PRF alone will not solve the problem. Harvesting PRF is technique sensitive, and serious consideration must be taken into account when buying a centrifuge ....... they don't all produce the same results.......as well make sure the vaccum tube used to collect the blood is glass and not plastic.
Carlos Boudet, DDS DICOI
2/25/2014
All the above comments have touched on some of the issues involved in similar situations, but the truth is that the doctor posting has provided very little information.
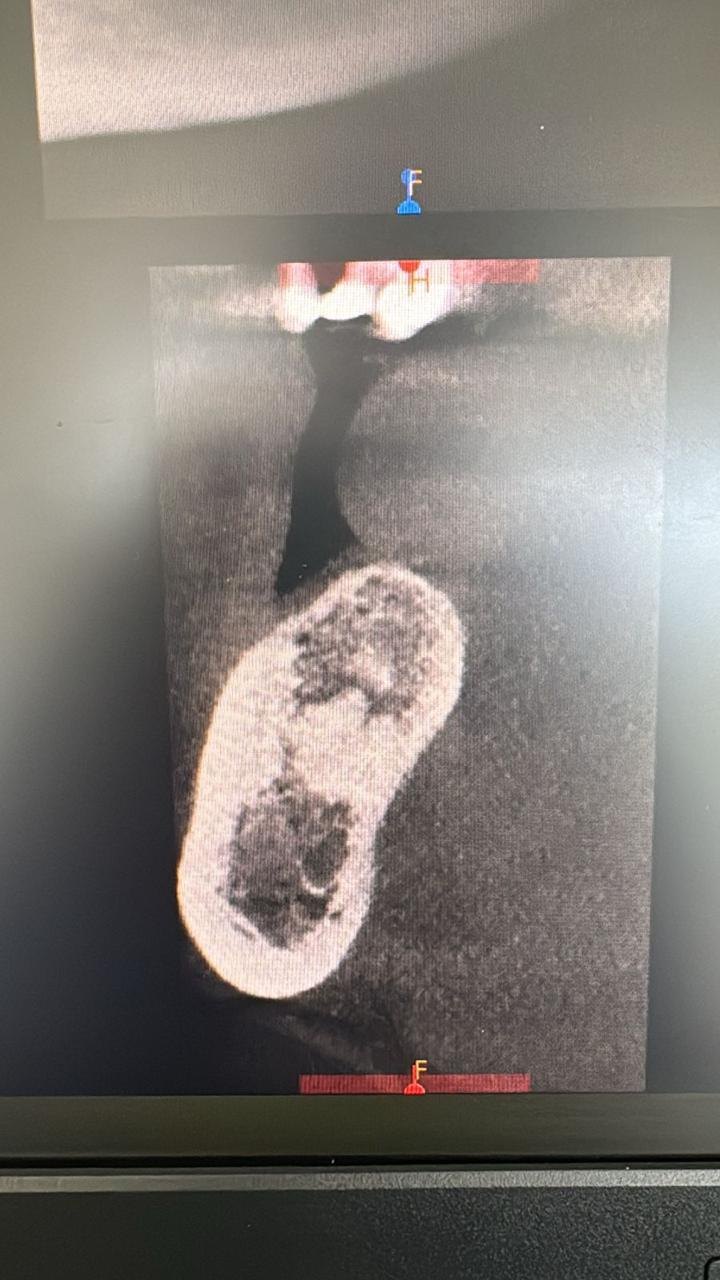
As a minimum, it would be good to have a pre-operative film and a post-op film showing the problem.
PRF is good, but it doesn't do things that are not biologically sound.
There has been no mention of where this implant is placed... An implant in the anterior region with the first thread exposed is a cosmetic failure.
Assuming the implant was placed at the proper depth, such an early bone loss could also be attributed to removing blood supply from the cortical bone if the implant was placed with less than 1.5mm of buccal an lingual bone.
Finally, the experience and skills necessary to detoxify and vertically augment the alveolar bone around this implant may be more than many of us can accomplish on a consistent basis.
Good luck!
Joseph Choukroun
2/26/2014
Carlos, well spoken !