Case: Ridge Augmentation with OSSIF-i Demineralized Sponge Strip
This case is presented by Dr. Kevin Frawley, DDS.
Pre-op (see case photos below)
This asymptomatic patient presented with an existing 3-unit hybrid Maryland bridge from #29-31 that had been in place for over 10 years. The esthetics were poor, and #31 showed signs of Periapical Radiolucency (PARL). After close monitoring for several months, the PARL worsened, and a buccal fistula developed. After treatment options were discussed, extraction and implant therapy was selected by the patient. Treatment aims included: improved esthetic spacing and contours, improved soft tissue health, and removal of any infection associated with the PARL.


![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/b047231a6b15f025118a3998821c4808.JPG)\#31 presented with vertical fracture and buccal fistula. Fixed bridge had been in place for 14 years. Treatment aimed to correct large buccal resorption on #30 area prior to implant placement. Extraction/Graft(see case photos below)
Extraction/Graft(see case photos below)
The existing prosthesis was removed without complication. After reviewing CBCT data, it was clear that there was not enough buccal-lingual bone thickness for successful implant placement in site #30. A full thickness flap was elevated and CBCT measurements were confirmed. #31 was sectioned, atraumatically extracted, the socket cleaned with a serrated curette, and grafted with Surgical Esthetics OSSIF-i Mineralized Cancellous .25-1mm particulate allograft.
A PTFE membrane was sized and placed on the buccal of #30, ensuring coverage past the margin of the defect in all directions. Decortication potholes were made with a high-speed round carbide bur, with copious irrigation, on the buccal of site #30. Once bleeding was induced, a Surgical Esthetics OSSIF-i Demineralized Sponge Strip allograft (10x6x7mm) that had been hydrated with sterile water for 10 minutes, was placed into the buccal defect. No fixation screws or pins were used. Surgical Esthetics OSSIF-i Mineralized Cancellous .25-1mm particulate allograft was placed surrounding the sponge. The ePTFE membrane then covered the graft material, and was tucked under the lingual flap. Nylon 5-0 monofilament interrupted sutures secured the graft and membrane in place. A simultaneous root-coverage procedure was done on #29, using a bonded-suture technique. We chose not to get primary closure, to preserve the vestibule and maintain the amount of keratinized tissue. ePTFE membrane and sutures were removed after 1 month.
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/9757b6265988f7da68b9e805c4d483a1.JPG)\#30 Pontic space with large resorption. #31 extracted atraumatically, and Surgical Esthetics particulate allograft in place.
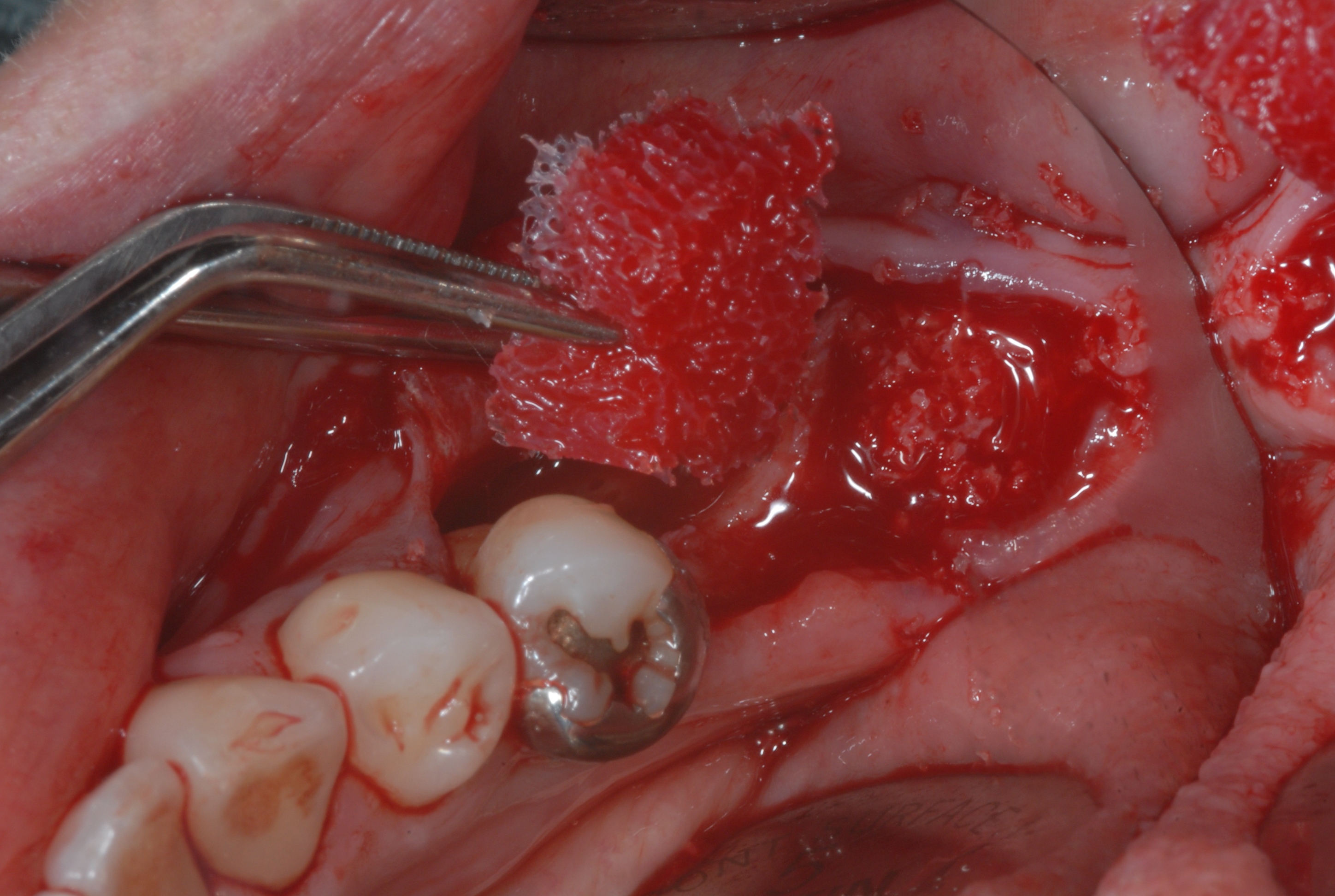
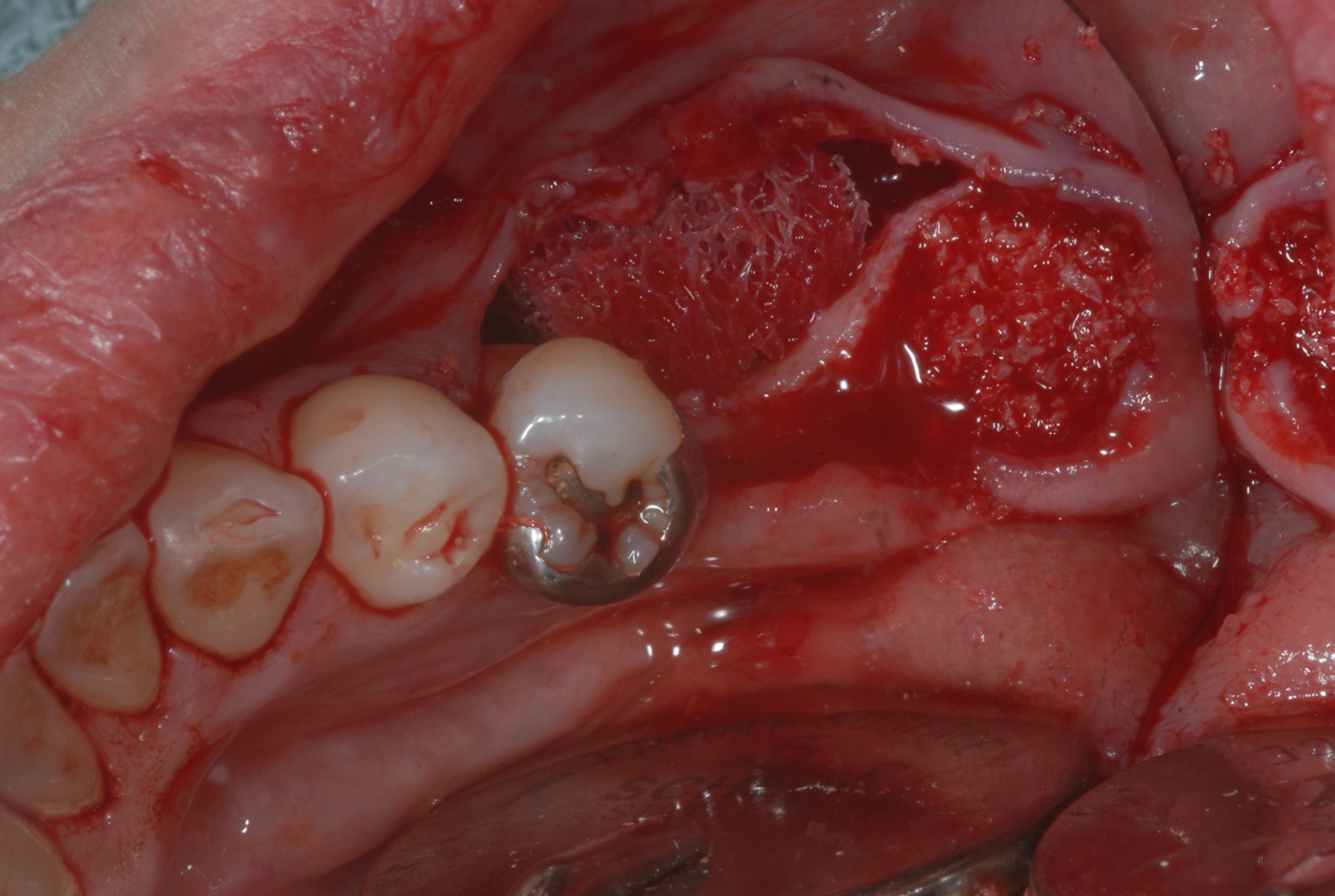
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/28a511d16ca0618eec97631af09c684d.JPG)Cortical perforations performed, and Surgical Esthetics allograft sponge strip being placed. Note blood absorption into allograft. Excellent for PRF technique
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/12ce36f63eadebceb6718a5c27745407.JPG)Initial sizing of sponge prior to membrane placement. Note that the sponge maintains space by tenting soft tissue. Fixation not required in this case.
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/892944b9d7a3f7f41fccb3b593b897b8.JPG)Cytoflex PTFE membrane in place, covering sponge and particulate allograft. (Some particulate placed to fill-in around sponge after membrane placed). Due to minimal vestibular and attached tissue, primary closure was not indicated.
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/79903f1f3ddc4b3abae5a3fa0c1d2c85.JPG)PTFE membrane removed at 1 month PO. Implant Placement (see case photos below)
Implant Placement (see case photos below)
After 5 months of healing, CBCT and surgical examination confirm readiness for implant placement. Compared to pre-op CBCT data, the Surgical Esthetics OSSIF-i Demineralized Sponge Strip allograft yielded >5mm of horizontal ridge augmentation! Two implants were placed and healing caps utilized. Papilla-saving suture techniques were employed.
![]At 4 month PO, tissue has matured into keratinized tissue.](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/f8a0748fee546795fa6483099683bd8d.JPG)At 4 month PO, tissue has matured into keratinized tissue.
![]Implants placed at 9 months as a single-stage procedure.](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/83a059d5dc4c96057187a952af3c4362.JPG)Implants placed at 9 months as a single-stage procedure. Restorative (see case photos below)
Restorative (see case photos below)
After 1 month, impression and restorative process commenced. Final screw-retained restorations were secured. All treatment goals were achieved. Three years later, the tissue, bone, and restoration/implant complexes are very stable.
![]Note improved keratinized tissue and buccal contour at impression appointment](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/21aeb0148f8e0d54b820e51d20221ac7.JPG)Note improved keratinized tissue and buccal contour at impression appointment
![]At 9 months PO, CBCT shows >5mm horizontal augmentation. (normally would wait >6 months to place implant](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/4e4b8228bc32763d33a1f469be0dfebe.jpg)At 9 months PO, CBCT shows >5mm horizontal augmentation. (normally would wait >6 months to place implant
![]Before and after comparison of soft tissue and restorations. Note increased attached tissue and root coverage on #29](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/9f84869c9087642d85e9cad890db86b4.jpg)Before and after comparison of soft tissue and restorations. Note increased attached tissue and root coverage on #29
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2017/04/befbcd2c6c1b6871ea92af6e67ffc91a.jpg)Before and after comparison of soft tissue and restorations. Note increased attached tissue and root coverage on #29About Dr. Kevin Frawley, DDS.
Dr. Kevin Frawley, D.D.S. is an exceptional person and a professional dedicated to helping his patients create the smile they were meant to have. He practices in Beverly Hills with his son, Dr. Shawn Frawley and his daughter, Dr. Michele Frawley.
He received his undergraduate degree from UCLA with a B.S. in Biology in 1977. He enjoyed being a Bruin so much that he completed his dental degree at UCLA as well in 1981. After a year residency at the Veterans’ Administration in Westwood, he established his private practice in cosmetic and implant dentistry in Beverly Hills. Dr. Frawley taught at the UCLA School of Dentistry for 15 years passing on his knowledge to the dentists of tomorrow.
Dr. Frawley is committed to the development of dentistry on all levels and is involved with both local and national dental associations. He is a member of the American Dental Association, California Dental Association and many other dental organizations. He is past president of the Beverly Hills Academy of Dentistry and past president of the Los Angeles Dental Society. Dr. Frawley served as a CDA delegate for over 25 years and as a trustee for the California Dental Association for 6 six years.
Dr. Frawley also lectures nationally and internationally on bone grafting and implants. He teaches live surgical courses as well that enable practicing dentists to gain the experience they need to feel confident to begin placing implants.
Dr. Frawley is the Founder and CEO of Surgical Esthetics, a regenerative material and education company.


















%5C#31){kind=link}
%5C#30){kind=link}
Cortical){kind=link}
Initial){kind=link}
Cytoflex){kind=link}
PTFE){kind=link}
At){kind=link}
Implants){kind=link}
Note){kind=link}
At){kind=link}
Before){kind=link}
Before){kind=link}