Would you use a short implant in this case?
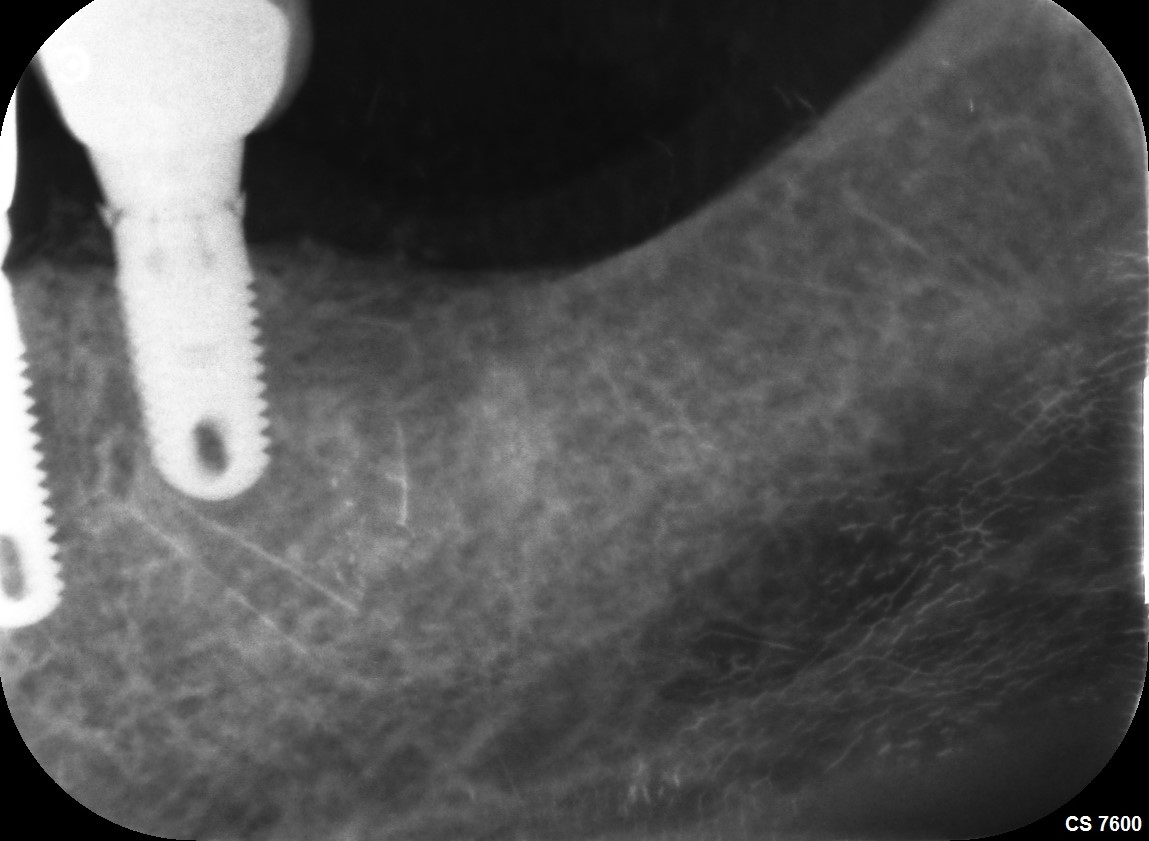
I would like to replace a lower right second bicuspid with an implant. The tooth is right over what appears to be 2 mental foramina, as can be seen in the radiograph. After extraction and grafting, there will be 8-9mm vertical bone height. I am not too familiar with Bicon-type shorter implants, but I feel like this maybe a good case for them. What do you recommend in this case? Oh I get by with a little help from my friends!




28 Comments on Would you use a short implant in this case?
New comments are currently closed for this post.
KK
1/18/2018
A bit risky, I would consider a bridge.
Mark Bourcier DMD
1/18/2018
I place Bicon exclusively. I think you need to see what the bone volume is after 4-5 months of graft healing. You could place a 4.5mm x 6.0 long here, but it is meant to be 2mm subcrestal, so you need an 8mm deep osteotomy, and I don't know if you are going to have that much to work with after the extraction. If you have good width, though, you could go quite short and fat, like a 4.5 x 5. I personally don't like risking a nerve injury. Be careful of your measurements before proceeding. A jury might ask "why didn't you do a bridge here. "
jeff
1/18/2018
You have a very nice BL width.
Any brand implant will do. 6 or 7 mm.
You could use a 5mm diameter implant. Plenty of contact surface.
jeff
1/18/2018
That,s the thing with Bicon. Short implant but 2mm subcrestal? A short 6mm implant takes 8mm depth?
Nice case for a regular Astrateck-Nobel-straumann-Bio-etc... 5MM wide X 6or 7mm length, to be determined on the CBCT after graft healing.
Ekaterina
1/18/2018
I had a similar case and would recommend to place the ceramic Maryland bridge
Dok
1/18/2018
"Modified" Maryland bridge ( they don't fall out, as the wings are internalized ).Done with minimal tooth preparation ( about the size of a small class 2 on each tooth ). Quick-easy-inexpensive. Patient will thank you for all of that.
Norris
1/24/2018
What material is the bridge made of? what cement? Do the Class II boxes need to be perfectly vertical, or are they prepped with a bit of taper? I'm interested in doing this, thanks!
Matt Helm DDS
1/24/2018
By the way, I think that in this case an inlay/onlay bridge is the ideal solution. I remain of the opinion that this is NOT an implant case, as I already stated in my original comment! The risks are too great.
Matt Helm DDS
1/27/2018
Norris, Dok is referring to what is accurately called an inlay bridge, or onlay bridge, not a “modified Maryland bridgeâ€. (Sorry Dok, there is no such thing as a “modified Maryland bridgeâ€, at least not in American terminology.â€) Have you never done an inlay or an onlay? If you haven’t here’s the shortest version I can give you, short of a lecture.
When preparing for an inlay or onlay bridge, you prep the abutment teeth just like you would for an inlay or an onlay, i.e.: standard class II preparations with at least 5 degrees of taper, flaring outwards in all directions from the inside towards the occlusal and the proximal. The preps are done with flared flat-head diamond burrs. In an inlay bridge, you just prepare a class II preparation inlay (with that 5 degrees of taper). In an onlay bridge you prepare the same class II preparation AND cuspal protection, so that the tooth cusps are also covered, just like in a standard onlay. There is a certain way to prepare the cusps, with a reduction of 1-1.5 mm, while preserving their basic shape so that the restorative material practically “wraps around the cusp†while also rebuilding it — you don’t just cut down the cusp flat. An onlay bridge is better because it protects the cusps and therefore protects the tooth from developing internal cracks or, against fracture of a whole cusp or wall. In most situations one should always choose an onlay bridge when possible. Another advantage of the onlay bridge in this case, considering the patient’s age and horizontal bone loss, is that the bridge cusps can be modeled in such a way (and the occlusion can also be adjusted) to have less stress on the abutment teeth during lateral excursions, thereby protecting the periodontium to minimize future horizontal bone loss.
The bridge can be made of any material, including metal, but the usual materials of choice are either lab-processed composites, porcelain, lithium disilicate, or zirconium. These bridges are usually bonded in, with the standard dentin/enamel bonding protocol and a composite cement. And yes, it can be made out of metal too but it will be very unsightly cosmetically. If metal, it’s cemented with either polycarboxilate cement if the teeth are vital, or zinc-oxyphosphate cement, if the teeth are non-vital. A metal bridge can also be bonded in (like composite or porcelain) but you’ll have to microetch the metal using a micro-etcher in order for the bonding material to stick to the metal. However, when bonding in a metal inlay bridge, consider also the possible need to remove it later — it will be much harder to remove. Once bonded in these inlay/onlay bridges CANNOT be removed by being tapped out with a sliding mallet, like ordinary bridges. Removal usually leads to destroying the inlay/onlay wings, regardless of the material used. There is also an entire protocol to insert them properly, as you MUST ensure that no composite cement gets trapped in the interproximal gingival embreasures and, you must finish and polish finely everywhere, including in the gingival embreasures. These bridges are not necessarily hard to do but they are finnickey, requiring attention to many details, much more so than standard crown & bridge. If you’ve never done this kind of bridge I suggest you first take a course on it. Otherwise, it will be much easier to do standard crown preparations and do a standard porcelain-fused-to-metal or zirconium bridge.
Matt Helm DDS
1/28/2018
Also, on the bicuspid you must absolutely use an onlay or a crown (definitely not an inlay) because it already has endo. Yes, a combination bridge consisting of a crown on the bicuspid and an inlay or onlay on the molar can be fabricated in the lab using any of the modern composites or porcelains. It's done quite often.
Greg Kammeyer, DDS, MS
1/18/2018
I'd place a Nobel 5.5mm Active that is 7mm. Keep in mind you want 2mm zone of safety away from the IAN.
Perioperry
1/18/2018
Best to do a fixed bridge here. No need to step into the stressful realm of trying to prevent or manage mental nerve paresthesia, or of dealing with a poor crown/root ratio after a restoration is placed on what would inevitably be a very short implant.
Dobs
1/18/2018
Am I missing something? There appears to be rampant periodontal disease everywhere based on radiographs provided. There also appears to be an endo failure. Unless these problems are addressed, it will not matter whose titanium you use.
Stephen Cave
1/18/2018
Yes i think you are missing something. I find your reply interesting.This is a senior citizen with generalized bone loss. Pocket depth and hygiene acceptable.The second bi is a goner if thats the apparent failing endo you are referring to. I generally appreciate constructive comments. Thank you
Perioperry
1/18/2018
No evidence from the images presented here of “rampant†periodontal disease. Bone levels may be somewhat reduced, but this is not diagnostic of active periodontal disease. The “endo failureâ€, if that’s what the widened PDL around the LR premolar is, is best managed in this case by removing the tooth.
BTL
1/18/2018
Yep. All day. Nobel Parallel 5x7
Bill Woods
1/18/2018
I would remove both premolars, graft and consider a much larger implant in 28 and if enough one in 29 area and possibly that is a double abutted implant bridge. Not enough bone for me with Perio as an added obstacle. Jm2c. Bill
Ed Dergosits
1/18/2018
There is only one premolar. The other premolar was extracted when orthodontic treatment was done decades ago. I would remove the tooth and place one implant. Short implant work fine. I used to think otherwise.
Timothy C Carter
1/18/2018
It is not necessary to place an implant for every missing tooth. People have survived for many years without the over utilization of titanium.
LSDDDS
1/19/2018
Agreed, pt. has two functional molars.
Extract, graft and reevaluate need to replace
Matt helm DDS
1/19/2018
I prefer the "3 mm from the IAN" rule. That said, it also looks like your implant would be positioned directly over the mental foramen, and in this particular case I feel that the mental foramen is placed too occlusaly for you to be able to effectively stay away from it. I've seen cases (not mine) where implants placed directly over the mental foramen caused inexplicable neuralgia that was intractable even after implant removal -- so bad, in fact, that the neuralgia symptoms persisted even after implant removal and lower cast partial was placed. And I agree with Mark Bourcier that a jury might ask you why you didn't place a bridge here.
Personally I'm in the bridge camp on this one. A composite or zirconium onlay bridge will do just fine. The patient will thank you for it, and your sleep will thank you!
Ted Lewis, DMD FICOI FAAI
1/19/2018
In any case, the typical load on and implant prosthetic is up to 5 times (the load) of a natural tooth. As long as that is figured in there are many great suggestions in these comments.
Semer
1/20/2018
Mental nerve transfer or transposition is not an option here?
Doc
1/20/2018
No not possible. The implant in this case would be placed superior to the mental foramen. You can't transfer / transposition the mental foramen.
Dr. Bill Woods
1/20/2018
Sorry I did not see all of the radiographs. I’m not thrilled about the periodontal condition medically or distally to the tooth in question. Is there mobility? Active periodontal disease?
Doc
1/20/2018
There are so many comments here about rampant periodontal disease. Perio disease is not diagnosed my bone loss but an active attachment loss. This may be stable perio, but on a reduced periodontium. Only the dentist can answer us through an accurate perio assessment.
Mohamed H Mohamed
1/23/2018
I don't know if you are a Bicon user but if the patient agrees to proceed after presenting all the risks. I would use Bicon 4x5mm even if you have enough BL width to make sure you are not encroaching on the buccal wall and to add bone graft in the gap left
you will need 1 mm subcrestal so the total length will be 6mm. in order to get the length try to engage the lingual wall by drilling at 2 mm crestal to the apex then redirect your pilot drill exactly as if you are doing an implant in the maxillary incisor
by doing so you will be away from the mental and your next drills will be away from the buccal plate
you can use any system with 6 mm length like ankylose for example
Don Rothenberg
1/27/2018
If an implant is the “patients†choice after completely explaining all and any risks, I would consider a Bicon 4.5x5 implant placed 1 mm subcrestal. Bicon can be placed 1-2 mm subcrestal, 2mm is not written in stone!
I believe the crown:root ratio is not a issue as Bicon has shown for years. I would also only use hand reamers as the original Bicon (DB) Implant was meant to be.
It is extremely important to discuss EVERTHING with the patient!
Would love to see the final result at some time.