Worth an Endo consult or straight to Implant ?
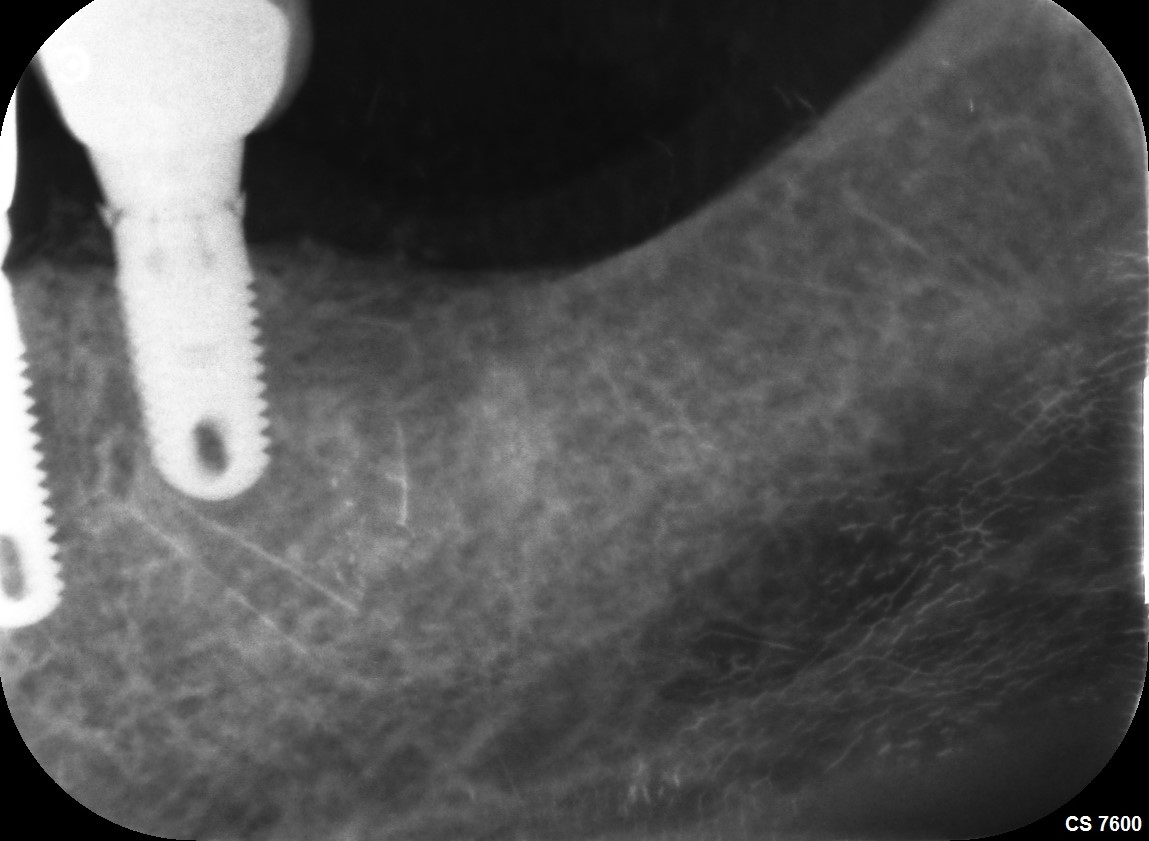
34 year old female patient presents for a consultation for tooth #30. Separated instrument in the M canals, large lucency extending around the MB continuous with the furcation and around the DB root. Pain to biting. Probing 15 mm straight to the apex from the straight buccal. Is this tooth worth sending for an endo consult or should I go straight to a dental implant?
 Probing 15 mm to apex
Probing 15 mm to apex Large lesion can be seen on CBCT ? Is this a crack?
Large lesion can be seen on CBCT ? Is this a crack? Separated instrument in mesials
Separated instrument in mesials
15 Comments on Worth an Endo consult or straight to Implant ?
New comments are currently closed for this post.
CRS
6/28/2013
If the RCT is 10-15 years old I would extract vs retreat, the 15mm buccal dehiscence is strongly suggestive of a fracture. What is going on with the second molar furcation area?
ttmillerjr
6/28/2013
I think enough has been invested in this tooth, poor prognosis whatever you try. I think I'd ext and get rid of that infection, then come back in seven weeks and graft or if you are comfortable the place implant and graft simultaneously.
Seth rosen
6/29/2013
It's gone. Why invest another $1500-$2500 on a very poor prognosis tooth. That kind if money, in my area, almost pays for the whole implant, post, and crown.
susan
7/2/2013
extract, but only because of the broken file.
Scott levy
7/2/2013
So this case was retreated (non surgically)and healed completely with 1-2 mm probing depths within 8 months! Have pictures and Radiographs but don't know how to post !
OsseoNews
7/2/2013
To Post photos go to: http://www.osseonews.com/post-case-photos-and-get-feedback/
Please be sure to use the same email you used to post the original case and be sure to include the original title of your case. Thank you.
Alejandro Berg
7/2/2013
Not worth the tome, effort or money, go for the socket preservation and later implant.
cheers
Rand
7/2/2013
Amen to extraction. Retreatment and long term prognosis very bad.
James Hastings
7/2/2013
Agree with previous posts. Extract, remove infected tissue, allow to heal, bone graft, allow to heal, place implant. It's not simple but it's predictable.
Dr. Gerald Rudick
7/2/2013
My comment might sound completely obnoxious..... but an opinion is only an opinion.
Years ago, when implants were unheard of and not being done.....every tooth was precious, and if we could not safe an entire tooth, then we would save a part of a tooth...hence we had hemisected molars supporting bridges very nicely...for years on end.
In this case, the roots are nicely spread apart.... if the patient is willing to try something a little different....what could be done is to extract the tooth......providing it does not fracture upon removal, then retrograde apicoectomies could be done to each root, while you are holding the tooth in your hand wrapped in a piece of gauze soaked n sterile saline, gently plane the root surfaces.
The socket is curreted, washed with citric acid, and rinsed with saline.
Prior to starting this procedure, draw two vials of whole blood and centrifuge for 12 minutes, and place the retrieved Platelet Rich Fibrin clot into the socket and the tooth replanted back in its socket.
You have created a natural implant.... the PRF is excellent as being pleuripotential, and can stimulate regrowth of the periodontal ligament.
I used to do this sort of thing more than 35 years ago with good results, when we did not have PRP or PRF.... the tooth would become solid again, and the pathology would disappear.......what did happen on occasion is that the body would regard the replanted tooth as a foreign body and begin to resorb it...but this could take years...so if your patient is willing..... go for it.... it is very inexpensive, and will cause no damage, and it will preserve the bone.
Gerry Rudick Montreal, Canada
dr.pradeep kumar .y.
7/3/2013
extract and curette the area completely and then immediate implant
tai
7/3/2013
it seems very clear that the tooth is hopeless , I guess due to fracture or crack at root or bifurcation.
anyway in new rct if you expand the canals you will have frcture in the future for sure.
so..... extraction and implant etc....
good luck
Dr Yawar Abidi
7/5/2013
I would suggest extraction as the tooth is associated with alot of problems.
Most probably its a cracked tooth, separated instrument, large buccal defect, radiolucencies around mesial and distal roots.
Completely curette the site and wait for six months before you place an implant.
Sam Jain DMD
7/16/2013
Flap less extraction -disinfection-immediate implant-bone graft-use the existing PFM to make screw retained temporary.
Px has solid furcation bone...very easy immediate case. You can get 50 -60 N torque.
It must be done.
No cuts, no sutures, only one Motrin next day. Awesome.
wes turnage
7/17/2013
straight to implant